Download
1 / 10
100 likes | 278 Views
CIMI. Member Survey. Survey Statistics. Survey sent to all 19 members : CDISC Canada Health Infoway CEN en13606 Association GE/Intermountain HL7 IHTSDO Kaiser Permanente Mayo Mitre MOHHoldings Singapore NEHTA (Australia) openEHR Results4Care SMART South Korea

E N D
CIMI Member Survey
Survey Statistics Survey sent to all 19 members : • CDISC • Canada Health Infoway • CEN • en13606 Association • GE/Intermountain • HL7 • IHTSDO • Kaiser Permanente • Mayo • Mitre • MOHHoldings Singapore • NEHTA (Australia) • openEHR • Results4Care • SMART • South Korea • Tolven • NHS England • US Departments and Agencies
Survey Statistics Responses received from 10 members • CDISC • Canada Health Infoway • CEN • en13606 Association • GE/Intermountain • HL7 • IHTSDO • Kaiser Permanente • Mayo • Mitre • MOHHoldings Singapore • NEHTA (Australia) • openEHR • Results4Care • SMART • South Korea • Tolven • NHS England • US Departments and Agencies
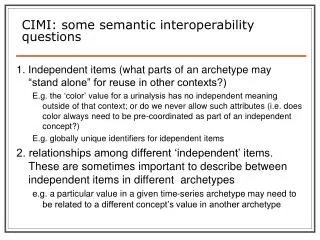
1. What is your biggest motivation for being part of CIMI? • (ALL) Our biggest motivation is to promote and to create real machine level interoperability of health information for patient care and other purposes eg (analytics for quality review, scientific / research concepts). We believe that the vision of CIMI models and tools hold the promise of enabling improved understanding of clinical meaning and context of exchanged information that will be beneficial for our patients, our caregivers, and the health system in which we operate. • (3) A network of shared intellectual capital around the table at the CIMI meetings. • (2) An organization that able to publish quality assured artefact libraries for worldwide use to support semantic interoperability. • ( 4) International harmonization • (2) Freely used and reduced cost of deploying electronic record systems . • (1) Harmonizes and accelerates work in progress in existing and new projects • (1) Clinical validation
2. What is the biggest de-motivator for you? • (4) The lack of funding which is making us less efficient as a group. • (3) Vested interests of individuals and/or individual groups. • Which lead to Modelling experts who cling to decisions they made years ago when the overwhelming consensus is against them. • ( 2) The different level of contributions of all voting members means that the risk is not shared, and the time required to move forward is significantly greater. • (2) Focus on a single approach to the exclusion of others, most notably Semantic Web and HL7 based approaches to modeling. If the needs of all these communities are not met equally then the vision of real interoperability will not be reached for all • (2) Need to ensure that we are truly international and not just serving the needs of one region or realm • (1) Consistently revisiting previous decisions • (1) The time it takes to produce a solution that includes biomedical research requirements that also may be too complex for most organizations to follow.
3. What business problem do you think that CIMI will solve for your organization? (1) • (3) Providing a single format for the representation of clinical information models so that • Users can share its models • Users can consume other models • Users can consume the models using commodity off the shelf tools • (3) Dealing with more complex sophisticated issues such as: • CDSS, reusability, • Standardization of detailed clinical information in EHR and HIE context. • Use of the clinical models in point of service systems and, in some cases, to establish interoperability between systems. They include CPOE, CDM, synoptic reporting, eReferral, discharge reports, and more • Data analytics from multiple systems • Bi directional semantic interoperability. • Share software and alerts • (3) A quality modelling process / development Improving the quality and usability of clinical models developed
3. What business problem do you think that CIMI will solve for your organization? (2) • (3) Better uptake of the individual organization’s ideas ( if the artifacts developed are aligned) • (2) The main business problem is that of real machine level data interoperability for clinical record information, across organizational boundaries, when documentation was originally captured using different information model paradigms. • (2) International harmonization hence reducing the costs of transformations between clinical models and also to computable models; and hence reducing the hurdles and costs of adoption • (1) encourage US vendors that potentially are developing for international; clinical models will expand their market and make their systems more useful to a broader market. • (1) That CIMI can provide a common way for both research and healthcare to represent semantics so that healthcare and research data can be interchanged and aggregated. This will also reduce the workload for defining scientific/research concepts in CDISC SHARE metadata repository.
4. What do you believe your organization can contribute to CIMI eg money, intellectual property, manpower or other resources?
5. Other Comments • 13606 Association - Tooling that produces OWL-DL statements should also be considered.Tooling that is fully driven by the ISO 13606 AOM is already available (LinkEHR). This means that LinkEHR can constrain any Reference Model (feature of 13606 AOM) and is in principle independent of the syntax used (presently LinkEHR uses ADL 1.4). LinkEHR can export to: ADL, XML, MindMap and OWL.
Next steps • The results to be sent to the remaining voting members and ask: • Are there other items they wish to contribute to questions 1 to 3 • Can they make any contributions such as noted in question 4 • Are they still interested in being a member. • IEC to review biggest de-motivator to see if there is anything that can be done.