Download
1 / 36
360 likes | 737 Views
FDA Review of Clinical Data Fragmin ® (Dalteparin sodium injection) for treatment of VTE in cancer patients. Medical Officer: Andrew Dmytrijuk, MD FDA/Center for Drug Evaluation and Research. Presentation. Regulatory Background “CLOT” Study ―Special Considerations Introduction to Questions.

E N D
FDA Review of Clinical DataFragmin®(Dalteparin sodium injection) for treatment of VTE in cancer patients Medical Officer: Andrew Dmytrijuk, MD FDA/Center for Drug Evaluation and Research
Presentation • Regulatory Background • “CLOT” Study―Special Considerations • Introduction to Questions
Regulatory Backgound Types of VTE Indications • Prophylaxis: • Primary prevention • Lower anticoagulant drug dose • Treatment: • Secondary prevention • Higher anticoagulant drug dose Differing risk: benefit considerations
Regulatory Background Drugs with VTE Indications • Prophylaxis: • Heparin (unfractionated) • Lovenox (enoxaparin sodium) • Arixtra (fondaparinux sodium) • Fragmin (dalteparin sodium) • Warfarin • Treatment: • Heparin (unfractionated) with Warfarin • Lovenox (enoxaparin sodium) • Arixtra (fondaparinux sodium) • Innohep (tinzaparin sodium)
Regulatory Background Drugs with VTE Indications • Specific population for prophylaxis • Broad population for treatment • Short term use of low molecular weight heparin drugs • At least two adequate and well controlled studies • Extensive historical experience with heparin/warfarin
Regulatory Background Guidance for Industry: Evidence of Effectiveness (May, 1998) • “Usual requirement for more than one adequate and well-controlled investigation…” or • “Demonstration of effectiveness by a single study of a new use, with independent substantiation from related study data” or • “Evidence of Effectiveness from a single study”…another study unethical or impossible
Regulatory Background Whether a single study + supportive dataorsingle study alone: “In all cases, it is presumed that the single study has been appropriately designed, that the possibility of bias due to baseline imbalance, unblinding, post-hoc changes in analysis or other factors is judged to be minimal and that the results reflect a clear prior hypothesis documented in the protocol.” ie., robust study findings
Regulatory Background Fragmin is currently approved for: • Deep Vein Thrombosis (DVT) prophylaxis in patients: • undergoing hip replacement surgery • undergoing abdominal surgery • at risk for thromboembolic complications due to severely restricted mobility during acute illness (5000 IU SC daily up to 8 - 14 days) • Ischemic complication prophylaxis in unstable angina and NQWMI when administered with ASA (10000 IU SC every 12 hrs up to 8 days) Not approved for treatment of DVT
Fragmin sNDA Proposed Indication and Dose • “Fragmin is also indicated for the extended treatment of symptomatic venous thromboembolism (VTE) (proximal DVT and/or PE), to reduce the recurrence of VTE in patients with cancer.” • 200 IU/kg (max. 18,000 IU) SC for 1 month followed by 150 IU/kg (max. 18,000 IU) SC for 5 additional months.
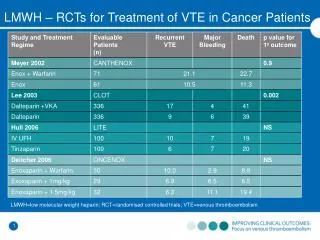
CLOT STUDY―Special Considerations “Randomized Comparison of Low Molecular Weight Heparin (Dalteparin) versus Oral Anticoagulant Therapy for Long Term Anticoagulation in Cancer Patients with Venous Thromboembolism” • Design Features • Results • Regulatory context
CLOT Design • International, multicenter • Open-label • 1:1 randomization • Fragmin vs OAC • Population: Cancer patients with acute proximal DVT and/or PE • Primary endpoint: comparison of time to first symptomatic recurrent VTE during 6 month study period
CLOT Design • Experimental (Fragmin group) Initial Rx - Fragmin 200 IU/kg SC qd x 1 month Extended Rx- Fragmin 150 IU/kg SC qd x 5 months • Control (OAC group) Initial Rx - Fragmin 200 IU/kg SC qd x 5-7d + OAC Extended Rx – OAC with INR 2-3 x 6 months
CLOT Design Features: • Open label • Study groups differed in anticoagulation monitoring • OAC group required regular blood INR monitoring • Potential impact upon symptom monitoring • “Symptomatic VTE” primary endpoint required survival―results susceptible to: • Death without VTE • Difficulty in VTE ascertainment near time of death • Initial Fragmin use in both study arms • Superiority to placebo/assumptions
CLOT Study Timeline & Protocol Changes • First patient enrolled: May 3, 1999 • September 13, 1999: Primary endpoint redefined from: Recurrent VTE & Major Bleeding to Recurrent VTE • Sample size readjusted: 1999 and 2001 • Last patient completed: April 9, 2002.
CLOT Study Results Baseline Characteristics • Balanced between study groups • Median age 64 (22-89) • 90% solid tumors • 75% stage IV • 10% no evidence of tumor
CLOT Study Results Subject Disposition
CLOT Study Results Primary Endpoint Result Log rank p = 0.002
CLOT Study Results Time to First Recurrent VTE
CLOT Study Results Time to First Recurrent VTE • Survival required to experience VTE symptoms • Mortality and VTE present competing risks • 40% mortality at six months • Death rate 3X greater than VTE rate • Imbalances in VTE-death categorical outcomes • VTE-free survival similar between study groups
CLOT Study Results Categories of Death & VTE Outcomes Subjects counted only once in each category
CLOT Study Results Categories of Death & VTE OutcomesDifferential Effects • Death followed a recurrent VTE: • Fragmin 6% vs OAC 12%; Δ = - 6% • Death without a recurrent VTE: • Fragmin 33% vs OAC 28%; Δ = + 5%
CLOT Study Results Categories of Death & VTE Outcomes • Inaccuracy in diagnosis of VTE near/at time of death may importantly impact results • VTE-free survival outcomes useful • - Straightforward clinical interpretation • - Resolves competing risk considerations
CLOT Study Results Time to VTE or Death Log rank p = 0.20
CLOT Study Results Other Exploratory Efficacy Analyses • “Time to treatment failure” (defined as time to recurrent VTE or discontinuation of study drug due to death) showed similar outcomes between study groups (log rank p = 0.65) • Post-hoc, exploratory subset analyses suggested no treatment effect among patients with: • nonmetastatic cancer • hematologic cancer • Hospitalization rates similar between study groups
CLOT Study Results Summary of Efficacy Finding Limitations • Robustness of primary endpoint called into question by: • Competing risks of death and VTE • Design features: differing patient management between study groups/symptom detection/open label • Variable results among sensitivity analyses
CLOT Study Results • Major Safety Observations • Study drug discontinuations due to death • Major bleeding • Thrombocytopenia • Liver enzyme/bilirubin elevations
CLOT Study Results • Study drug discontinuation due to death • 17% Fragmin vs 7% OAC, • however • Overall mortality similar • 39% Fragmin 41% OAC
CLOT Study Results Death rates by month of study drug exposure median 176 days Fragmin; 167 days OAC
CLOT Study Results • Imbalance in study drug D/C due to death • Possible safety signal • Causes: • - imbalance in study drug exposure • - variations in patient management • - drug effect
CLOT Study Results Major Bleeding: 6% Fragmin vs 4% OAC
CLOT Study Results • Thrombocytopenia • Liver enzyme/bilirubin abnormalities
CLOT Study Results Summary of Safety Findings • 1. More Fragmin patients discontinued study drug due to death • Fragmin group experienced numeric excess in: • Major bleeding • Thrombocytopenia • Liver enzyme/bilirubin elevations
CLOT Overall Summary Design limitations: - open label - redefined primary endpoint - differing anticoagulation management in study groups - primary endpoint required survival Efficacy: - treatment effect confounded by competing risks of death and recurrent VTE - treatment effect for Fragmin evidenced in the first month; no further gain in months 2-6 Safety: - excess study drug discontinuation due to death, - small excess in major bleeding, thrombocytopenia, liver test abnormalities
CLOT Study in Regulatory Context • CLOT is a single study with important limitations in data interpretation • Short term regimens of Fragmin have proven efficacy and safety in other populations when used for VTE prophylaxis • Proposed indication and dose regimen is only for “cancer patients” with VTE • Safety and efficacy of proposed dose regimen has not been confirmed for broader population of patients with VTE
Topics for Questions: • Assessment of CLOT safety findings • Robustness of CLOT study efficacy findings • Potential label considerations • Potential need for additional studies