Download
1 / 19
190 likes | 491 Views
Iodine-131 Therapy and the Dialysis Patient. M.J. Bohan and R.L. Richardson Yale-New Haven Hospital Radiation Safety Office. The Problem. Thyroid cancer and hyperthyroid patients with renal failure present a number of radiation safety and medical physics challenges

E N D
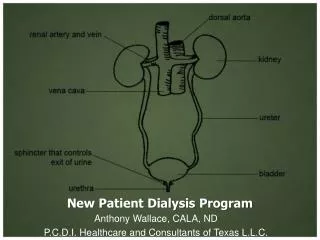
Iodine-131 Therapyand the Dialysis Patient M.J. Bohan and R.L. Richardson Yale-New Haven Hospital Radiation Safety Office
The Problem • Thyroid cancer and hyperthyroid patients with renal failure present a number of radiation safety and medical physics challenges • Unfortunately, there is not a lot of published sources of information in the literature that address the issues presented by these patients YNHH RSO - HPS 2006
Health Physics Issues • Potential for increased occupational exposures • Potential for contamination control and waste disposal issues • Early patient release issues - dose to family and the public YNHH RSO - HPS 2006
Medical Physics Issues • How much longer in advance should you recommend iodine dietary restrictions and removal of replacement hormone? • Uptake studies may be misinterpreted due to poor systemic washout at 24 - 48 hrs • Altered excretion kinetics results in greatly increased whole body dose YNHH RSO - HPS 2006
Case Study Number 1 • Female thyroid cancer patient with end stage renal disease on hemodialysis • Written directive - Administer 5.6 GBq (152 mCi) • Hemodialysis on regular schedule at 48 hrs post administration • Patient isolated at hospital for first two dialysis sessions and then was followed as an outpatient for the next week YNHH RSO - HPS 2006
Patient WB ∞ Dose Estimates MIRD - Pamphlet 11 (1975), I-131 (TB <-- TB), 9.9E-6 rad/uCi-hr YNHH RSO - HPS 2006
Case Study Number 2 • Two years later, same patient, now on peritoneal dialysis • Written directive - Administer 11 GBq (296 mCi) • Peritoneal dialysis on regular schedule at home • Patient isolated dialysis wastes in garage • CAPD every 4-6 hours during the day • NIPD at night only, for first two days • After day 2, CCPD continuously (CAPD - Continuous Ambulatory Peritoneal Dialysis) (NIPD - Nocturnal Intermittent Peritoneal Dialysis)(CCPD - Continuous Cycle Peritoneal Dialysis) YNHH RSO - HPS 2006
Patient WB ∞ Dose Estimates MIRD - Pamphlet 11 (1975), I-131 (TB <-- TB), 9.9E-6 rad/uCi-hr YNHH RSO - HPS 2006
Case Study Number 3 • New male patient on peritoneal dialysis with about 15% of normal renal function • Written directive - Administer 1.2 GBq (31.3 mCi) • Peritoneal dialysis on regular schedule at home • Patient isolated dialysis wastes on porch • NIPD at night only YNHH RSO - HPS 2006
Hours YNHH RSO - HPS 2006
Patient WB ∞ Dose Estimates MIRD - Pamphlet 11 (1975), I-131 (TB <-- TB), 9.9E-6 rad/uCi-hr YNHH RSO - HPS 2006
Lessons Learned • If you give a dialysis patient a dose which would be appropriate for a normal patient, the whole body dose is extremely high • Because the I-131 continues to re-circulate in dialysis patients, you should be able to titrate the administered dose based on the calculated whole body dose and lower their dose without compromising their thyroid uptake • If patients have partial kidney function, you should take it into account when calculating the adjusted dose • Reducing the administered dose also helps with patient release issues YNHH RSO - HPS 2006
Consider Changing the Hemodialysis Scheduling • Modification of the hemodialysis schedule will dictate the administered dose • Schedule 1: 48 hrs post administration, MWF • Schedule 2: 48 hrs @ 24 hr post adm, TThSaMWF • Schedule 3: 24 hrs @ first 3 days then release from isolation with outpatient hemodialysis on Sa, then back to normal MWF YNHH RSO - HPS 2006
Estimated Whole Body Doses for 100 mCi Rx Normal Pt. - 0.11 Gy 48 hr @ 48 hr - 0.80 Gy (14%) 48 hr @ 24 hr - 0.59 Gy (19%) 24 hr @ 1st 3days - 0.47 Gy (23%) Mon Wed Fri Sun Fri Sun Tue Thur YNHH RSO - HPS 2006
Contamination/Waste Issues • Hemodialysis systems are self contained and use copious amounts of water to wash the blood. Residual contamination levels are usually low and easily cleaned up. Cartridges and tubing will retain low levels of activity and should be held for decay YNHH RSO - HPS 2006
Occupational Dose Issues • Hemodialysis nurses must stay close to the dialysis machine and service it periodically • You need to train them in time and distance controls to minimize their occupational dose • Measured Occupational Doses • 5.6 GBq (152 mCi) on in-patient hemodialysis • First Dialysis - Nursing Dose 18 mrad • Second Dialysis - Nursing Dose 42 mrad YNHH RSO - HPS 2006
References Jimenez, R.G., et al., Iodine-131Treatment of Thyroid Papillary Carcinoma in patients Undergoing Dialysis for Chronic Renal Failure: A Dosimetric Method, Thyroid, Vol. 11, NO. 11, 2001 Mars, D.R., et al, Iodine Retention and Thyroid Dysfunction in Patients on Hemodialysis and Continuous Ambulatory Peritoneal Dialysis, Am. J. Kidney Dis., June 1986, 7(6):471-6) Magne, N., et al, Disposition of Radioiodine 131-I therapy for Thyroid Carcinoma in a Patient with Severely Impared Renal Function on Chronic Dialysis: A Case Report, Jpn. J. Clininal Oncology 2002; 32(6) 202-205 Kaptein, E.M., Radioiodine Dosimetry in Patients with End-stage Renal Disease Receiving Continuous Ambulatory Peritoneal Dialysis Therapy, J Clin Endocrinol Metab. 2000 Sep;85(9):3058-64 Sisson, J.C., Practical Dosimetry of 131-I Patients with Thyroid Carcinoma, Cancer Biotherapy & Radiopharmaceuticals, Vol. 17, No. 1, 2002 Thomas, S.R., Options for Radionuclide Therapy: From Fixed Activity to Patient-Specific Treatment Planning, Cancer Biotherapy & Radiopharmaceuticals, Vol. 17, No. 1, 2002 Kaptein, E.M., Radioiodine Dosimetry in Patients with End-Stage Renal Disease Receiving Continuous Ambulatory Peritoneal Dialysis Therapy, The Journal of Clinical Endocrinology & Metabolism, Vol. 85, No. 9, 2000 YNHH RSO - HPS 2006