Download
1 / 41
410 likes | 1.15k Views
支架内血栓 In-Stent Thrombosis. 北京大学第一医院 李建平. Definite/Confirmed (肯定的) Acute coronary syndrome AND [Angiographic confirmation of thrombus or occlusion OR Pathologic confirmation of acute thrombosis] Probable (可能的) Unexplained death within 30 days

E N D
支架内血栓In-Stent Thrombosis 北京大学第一医院 李建平
Definite/Confirmed (肯定的) Acute coronary syndrome AND [Angiographic confirmation of thrombus or occlusion OR Pathologic confirmation of acute thrombosis] Probable (可能的) Unexplained death within 30 days Target vessel MI without angiographic confirmation of thrombosis or other identified culprit lesion Possible (不能排除的) Unexplained death after 30 days ARC 支架内血栓定义
支架内血栓的预后 Similar mortality observed for SES and BMS thrombosis Pooled Data from RAVEL, SIRIUS, C-SIRIUS, E-SIRIUS
支架内血栓发生时间 ST = stent thrombosis; SAT = subacute stent thrombosis; LST = late stent thrombosis; VLST = very late stent thrombosis. Adapted from Bhatt. J Invasive Cardiol. 2003;15(suppl B):3B.
DES 支架内血栓与抗凝、抗血小板治疗 Bare Metal Stent ASA und Anticoagulation ASA und Ticlopidine Stent Thrombosis (%) ASA und Clopidogrel Prasugrel? ASA = Acetylsalicylic acid DES: Drug-eluting stent
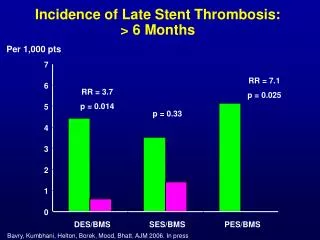
BMS支架内血栓发生率 Early 1.2% (N=71) Late 0.4% (N=24) Study population 1995-2002 -6,058 patients undergoing PCI with BMS 10 N Wenaweser P et al. EHJ 2005 8 0 30 60 600 120 Days 6 4 2 Stent Thrombosis (%) 0 N=1,191 N=1,855 N=361 N=6,058
Late ST 61 pts (40%) Early ST 91 pts (60%) DES肯定的ST发生率:Bern - Rotterdam Cohort Study Daemen, Wenaweser et al. Lancet 2007;369:667-78 N=8146 0.6% / year Incidence density: 1.3 / 100 patient years
DES肯定的ST发生率:Bern-Rotterdam Cohort Study @ 4 Years Wenaweser P et al. J Am Coll Cardiol 2008, 52, 1134- 5 192 definite ST cases 4 3.3% 0.53% (95% CI=0.44-0.64)/ year 3 Cumulative incidence, % 2 Incidence density 1.0 / 100 pt years 1 0 0 1 2 3 3.5 4 Time since PCI in years
DES肯定的支架内血栓发生率:Bern-Cohort Study @ 5 Years Wenaweser P et al. ESC 2008 0.52% (95% CI=0.42-0.62)/ year between 30 days and 5 years
DES vs BMSA cohort of 9,175 patients treated with either BMS or DES (SES or PES), all patients with angiographically documented ST were identified as cases Adjusted Resultswith interaction terms for time since PCI Early period: 0-30 days OR 0.59, 95% CI .35 - 1.01 Late period: 31-180 days OR 0.52, 95% CI .16 – 1.75 Very late period: > 180 days OR 9.4, 95% CI 2.56 – 34.70 0-30 days Time after PCI 31-180 days >180 days FavoursDES Favours BMS Favors DES Favors BMS .1 .2 .5 1 2 5 10 20 50 100 .1 .2 .5 1 2 5 10 20 50 100 Odds Ratio Odds Ratio Wenaweser et al. ACC 2007
Very Late ST > 1 Year (Per Protocol) Sirolimus-Eluting Stent Paclitaxel-Eluting Stent % % P=0.75 P=0.30 P=0.03 P=0.02 Kastrati A et al. NEJM 2007;356:1030-9 Stone G et al. NEJM 2007;356:998-1008
4-year HR 1.06 [0.57, 1.95] P = 0.86 3-year HR 0.90 [0.47, 1.73] P = 0.75 2-year HR 0.86 [0.40, 1.87] P = 0.71 1-year HR 1.12 [0.46, 2.76] P = 0.01 SES 4.2% PES 3.9% SIRTAX – Definite ST @ 4 Years Windecker S et al ESC 2008 3.7% 2.8% 2.0% 3.4% 2.4% 1.8%
CYPHER TAXUS Overall Incidence of ST with DES ENDEAVOR XIENCE BIOMATRIX 3 1.9 1.6 2 2 1.4 1.8 % 1 1.1 0.8 0.8 0.7 1 0.8 0.5 0.5 0.6 0.4 0.3 0.2 0 0 ARTS II SIRTAX TAXUS II REALITY ISAR-DM TAXUS V SIRTAX ISAR-DM SIRIUS TAXUS IV TAXUS VI C-SIRIUS E-SIRIUS REALITY Spirit III Leaders Endeavor I Endeavor II
High Risk of ST in All-Comer Patient Population and STEMI Patients %
Stent Design/Length Polymer Surface Drugs Intervention Residual Dissection Incomplete Stent Apposition Antithromobotic Medication Lesion Vessel Size Thrombus 支架内血栓的病因 Patient Genetic Polymorphism Reduced LV-EF Acute Coronary Syndrome Hematology Disorder Drugs Resistance Drug-drug Interaction Duration of Antiplatelet Treatement STENT THROMBOSIS Vessel Reaction Vessel Remodeling Hypersensitivity Reaction Delayed Healing
早期支架内血栓的预测因素:残留夹层/撕裂 Bare Metal Stents MACE @ 30 days Schühlen H et al. Circulation 1998 Drug-Eluting Stents MACE @ 30 days Biondi-Zoccai G et al. EHJ 2006 Residual Dissection: Independent Predictor of MACE (OR=2.9) P=0.01 % P=0.01 N=2,894 N=2,418
早期支架内血栓IVUS预测因素With the Use of Sirolimus-Eluting StentsFujii K et al. J Am Coll Cardiol 2005;45:995-8 Minimal Stent CSA Stent Expansion Residual Stenosis mm2 % P<0.001 P<0.001 P<0.001 Stent Underexpansion and Residual Reference Segment Stenosis: Independent Predictors of Early Stent Thrombosis!
支架内血栓预测因素药物反应异常Wenaweser P et al. JACC 2005; 45(11):1748-52
服药后血小板活性与DES ST的关系Buonamici P et al JACC 2007 p<0.001 p<0.001 p=ns p<0.001
过早停用抗血小板药物是支架内血栓的重要预测因素过早停用抗血小板药物是支架内血栓的重要预测因素 OR=89.8 (29.9-270) HR=19.2 (5.6-65.5) OR=4.8 (2.0-11.1) HR=13.7 (4.0-46.7) Odds/Hazard Ratio Iakovou et al JAMA 2005 Park et al Am J Card 2006 Kuchulakanti et al Circulation 2006 Airoldi et al Circulation 2007
支架内血栓发生时的抗血小板治疗 Bern-Rotterdam Cohort Study @ 5 YearsWenaweser P et al. ESC 2008
支架内血栓的预测因素-支架长度 OR=1.03 (1.00-1.05) OR=1.02 (1.00-1.04) OR=1.01 (1.00-1.03) OR=1.08 (1.06-1.1) OR=2.75 (1.55-4.88) Odds Ratio Iakovou et al JAMA 2005 Park et al Am J Card 2006 Machecourt et al JACC 2007 De la Torre et al JACC 2008 Airoldi et al Circulation 2007
支架内血栓的预测因素-分叉病变 OR=12.9 (4.7-35.8) OR=6.4 (2.9-14.1) OR=4.4 (2.0-10.0) OR=2.4 (1.1-5.6) Odds Ratio Roy et al J Interv Card 2007 Ong et al JACC 2005* Iakovou et al JAMA 2005 Kuchulakanti et al Circulation 2006 *in setting of AMI Joner et al JACC 2006
支架内血栓的预测因素-ACS OR=12.4 (1.7-89.7) OR=2.3 (1.3-4.0) OR=1.8 (1.1-2.7) HR=2.6 (1.3-4.9) Odds/Hazard Ratio De la Torre et al JACC 2008 Park et al Am J Card 2006 Daemen et al Lancet 2007 Urban et al Circulation 2006
Impact of Thrombus Burden on Risk of ST With DES in Patients With STEMISianos G et al. J Am Coll Cardiol 2007;50:573-83 Independent Predictors of ST Variable Hazard Ratio 95% CI Age 0.6 0.4-0.8 Index ST 6.2 2.1-18.9 Bifurcation 4.1 1.6-10.0 Thrombectomy 0.1 0.01-0.8 Large thrombus 8.7 3.4-22.5
支架内血栓的预测因素-糖尿病 OR=2.0 (0.8-4.9) HR=1.75 (1.0-3.0) OR=2.8 (1.7-4.3) OR=2.7 (1.4-5.2) HR=3.7 (1.7-7.9) HR=2.0 (1.1-3.8) HR=2.2 (1.1-4.3) Odds/Hazard Ratio Kuchulakanti Circ 2006 Urban Circ 2006 Machecourt JACC 2007 Iakovou JAMA 2005 Daemen Lancet 2007 Iijima Am J Card 2007 De la Torre JACC 2008
晚期支架内血栓的可能原因 • Chronic inflammatory reaction to the polymer or drug • Hypersensitivity to the polymer or drug • Failure of stents to completely reendothelialize completely • Late incomplete stent apposition • Disease progression
获得性晚期支架贴壁不良 Baseline 8 mo follow-up SIRIUS Trial: 7/80 (8.7%) patients, no 12-month MACE Ako J. et al. JACC 2005;46:1002-5
DES后病生理机制 Abnormal Vasomotion Delayed Healing Endothelialization Joner et al. JACC 2006 Togni et al. JACC 2005 Delayed Endothelialization Vessel Remodeling Kotani et al. JACC 2006 Cook et al. Circulation 2007
支架内血栓的预防 • 高危病人的辨认 • 避免过度支架 • 长支架, 分叉支架, 支架重叠 • 支架植入的理想结果 • 无残留撕裂/夹层 • 支架膨胀良好 • 增加抗血小板治疗的有效性 • 高危病人评估抗血小板药物的反应性 • 再狭窄低危病人中使用BMS
FDA DES Panel Meeting 专家共识 • There is an increase in “very late” (>1 yr) stent thrombosis associated with current DES • ~2-4 per 1000 pts per year (? continous hazard, ? patient and lesion predictors) • Data from multiple sources indicate thatDES are associated with delayed healingresponses and increased inflammation • The causes of late DES thrombosis are multi-factorial; device, procedural, and patientfactors (often multiple = perfect storm)
FDA DES Panel Meeting 专家共识 • There may be a link between post-DES reduced neo-intimal hyperplasia (late loss) and delayed late healing responses which contributes to late stent thrombosis • DES stent thrombosis is highly definition dependent; need for revised standardizeddefinitions and adjudication methods (ARC) to facilitate inter-study comparisons
专家共识 • “Off-label DES use – increased incidence of late DES thrombosis and death/MI cw “on-label”, butinadequate controls; results inconsistent! • Few RCTs (underpowered); FDA sanctioned registries = insufficient sample size and FU, represents major data gap and source of concern • Large population studies (SCAAR) fraught with methodologic flaws (e.g. risk adjustment issues)
专家共识 • Duration of dual anti-platelet therapy should extend beyond the present product labels • One year is reasonable compromise (esp. for“off-label” DES use) • Must balance against the increased risk ofbleeding with dual anti-platelet therapy • Additional studies immediately required tobetter clarify optimal anti-platelet therapy
专家共识 • Assess patient and lesion characteristics to establish restenosis risk profile • Determine relative value of DES vs. BMS inevery patient (no more “unrestricted” use) • Consider both on-label and off-label situations (ironically, off-label use scenarios may be more compelling) • Increased restenosis risk = favor DES • Increased safety concerns = favor No DES
专家共识 • Assess patient factors which may preclude long-term (at least one year) dual AP therapy • Planned or possible intercurrent surgery • Bleeding Hx or tendencies • Other concomitant medications (e.g. coumadin) • Socio-economic factors which may affect Plavix compliance
专家共识 • Consider alternatives to DES, if risk-benefit assessments prove unfavorable • CABG – unprotected LM disease, complex MVD (esp. diabetics), recurrent ISR (esp. VBT) • BMS – Plavix dependence concerns, large (>4mm diameter) vessels, ? AMI pts, ? low restenosis risk lesions • Balloon PCI – sidebranch in bifurcations (provisional stent only), small vessels in distal locations
专家共识 • Optimize DES implantation techniques • Adequate lesion preparation (pre-dilatation) • High pressure implantation methodologies (like previous BMS strategies) • Avoid undersizing and inflow/outflow obstruction (mod stenoses or dissections) • Implant stent edges into normal references segments • Consider IVUS guidance (esp. LAD)
专家共识 • Careful explanations and open communication with patients and families • Careful pre-treatment history • Discussion with EVERY pt re: risks and benefits of DES vs. alternative therapies • Ongoing (post-Rx) communication and careful FU re: dual AP compliance (instructions = NO Plavix discontinuation without MD approval)!
DES 风险 &获益 • 治疗1000个病人可以预防100个再狭窄 • 同时可以预防10个再狭窄相关的心肌梗死 • 可能会因为晚期支架内血栓增加5个心肌梗死 • 获益>风险