Download
1 / 23
230 likes | 386 Views
Emergency Contraception: Plan B through Z. Legislative Advocacy Noon Conference Melissa Woods PGY-2. Teen Pregnancy… An Introduction. Each year, almost 750,000 women aged 15-19 yrs become pregnant Two thirds of this occurs among 18 – 19 yr olds This rate has declined 40% from 1990 – 2005

E N D
Emergency Contraception:Plan B through Z Legislative Advocacy Noon Conference Melissa Woods PGY-2
Teen Pregnancy… An Introduction • Each year, almost 750,000 women aged 15-19 yrs become pregnant • Two thirds of this occurs among 18 – 19 yr olds • This rate has declined 40% from 1990 – 2005 • Historic low in 2005 70.6 per 1,000 women 15 – 19 yrs • Increased 3.5% from 2005 - 2006 • Eighty-two percent of teen pregnancies are unplanned; they account for about 20% of all unintended pregnancies annually • Of teenage pregnancies: 57% end in live births, 29% end in induced abortion, and 14% end in miscarriage or stillbirth • Teen pregnancy rates are much higher in the US than in many other developed countries • US rates are twice that of Canada and England, eight times as high as Japan, and ten times higher than France and Sweden
In Your Neighborhood… • Each year, almost 30,000 New York City teens become pregnant each year • In New York City, rates for teenage pregnancy far exceed the national averages • 99.4 per 1000 females aged 15 – 19 yrs • 29% higher than the US rate • Highest reported rates in the Bronx • 137.2 per 1000 females aged 15 – 19 yrs • Forty percent of all pregnant teens in NYC had been pregnant before • Of NYC teen pregnancies: • 41% live birth, 56% abortion, 3 % miscarriage
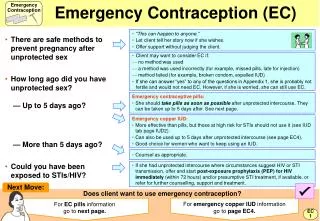
Emergency Contraception • The use of hormonal medications after sexual intercourse to prevent pregnancy • Indications: • Unprotected sexual intercourse • Underprotected sexual intercourse • Condom breaks or slips / diaphragm or cap dislodged • Two or more OCPs are missed • One or more progestin-only pills is missed • A depo-provera shot is 2 or more weeks late • The transdermal patch is detached for 24 hrs or longer • The vaginal ring is removed for 3 hrs or longer • Vaginal spermicide is used alone
The So-called“Morning After Pill” • Progestin + Estrogen • Preven, many combination OCPs • Progestin Only • Plan B, Plan B One Step, Next Choice • Antiprogestins • Mifepristone, Ulipristal
Progestin + Estrogen ECs • Preven • approved by the FDA in 1998 • removed in 2004 due to studies revealing that progestin-only pills were more effective and had a better side effect profile • Many brands of daily birth control can be used for emergency contraception and are approved for off-label use by the FDA • Effectiveness: 56 – 89%
Brand Company Pills per Dose EthinylEstradiolLevonorgestrel per Dose (μg) per Dose (mg) Progestin-only pills: take one dose Plan B Teva 1 white pill 0 1.5 One-Step Next Choice Watson 2 peach pills 0 1.5 Combined progestin and estrogen pills: take two doses 12 hours apart Alesse Wyeth 5 pink pills 100 0.50 Aviane Teva 5 orange pills 100 0.50 CryselleTeva 4 white pills 120 0.60 EnpresseTeva 4 orange pills 120 0.50 Jolessa Teva 4 pink pills 120 0.60 Lessina Teva 5 pink pills 100 0.50 LevlenBerlex 4 light-orange pills 120 0.60 Levlite Berlex 5 pink pills 100 0.50 Levora Watson 4 white pills 120 0.60 Lo/Ovral Wyeth 4 white pills 120 0.60 LoSeasoniqueTeva 5 orange pills 100 0.50 Low-Ogestrel Watson 4 white pills 120 0.60 Lutera Watson 5 white pills 100 0.50 Lybrel Wyeth 6 yellow pills 120 0.54 Nordette Wyeth 4 light-orange pills 120 0.60 Ogestrel Watson 2 white pills 100 0.50 Ovral Wyeth 2 white pills 100 0.50 Portia Teva 4 pink pills 120 0.60 Quasense Watson 4 white pills 120 0.60 SeasonaleTeva 4 pink pills 120 0.60 SeasoniqueTeva 4 light-blue-green pills 120 0.60 Sronyx Watson 5 white pills 100 0.50 Tri-LevlenBerlex 4 yellow pills 120 0.50 Triphasil Wyeth 4 yellow pills 120 0.50 Trivora Watson 4 pink pills 120 0.50
Progestin-Only Ecs • The only pills available specifically for emergency contraception in the United States • Plan B (1999) • Directions on package insert: one 0.75 mg dose within 72 hrs after unprotected intercourse and a second 0.75 mg dose 12 hrs later • 2002 WHO study found that progestin only ECs can be taken in one dose of 1.5 mg and that they can be taken up to 120 hrs after intercourse • There is a statistical decline in effectiveness with delayed use • Plan B One Step (2009) • Directions on package insert: one 1.5 mg tablet as soon as possible within 72 hrs after unprotected intercourse • Next Choice (2009) • Directions on package insert: same as Plan B above • Estimates of effectiveness 59 – 94%
International Alternatives • Antiprogestins • Progesterone receptor modulators • First generation • Mifepristone – aka. RU-486 • FDA Approved for use for early first trimester medical abortions (2000) • In other countries, used as emergency contraception in much lower doses than those used for abortion (10 vs. 100 mg) • Has the potential to disrupt a pregnancy after implantation within the uterine lining • Second generation • Ulipristal - aka. ellaOne (Oct 2009) • Only available in Europe • Labeled use: one 30 mg pill taken within 5 days of unprotected intercourse • Recent study comparing levonorgestrel with ulipristal suggests that ulipristal is at least as efficacious as levonorgestrel
Mechanism of Action • Primarily inhibits ovulation, disrupts follicular development, and/or interferes with the maturation of the corpus luteum • Plan B taken prior to the day before a woman’s LH surge suppresses the surge completely no ovulation • When Plan B is taken closer to or during the LH surge, it blunts or delays the surge and renders the ova resistant to fertilization • Early suggested histological/biochemical alterations of the endometrium, thereby impairing receptivity to implantation • More recent studies have demonstrated little to no effect on the endometrium • Other suggested mechanisms include alteration of sperm or egg transport, interference with fertilization, and/or cervical mucus changes • Have not been verified by clinical data • ECPs do not interrupt an established pregnancy that has already implanted in the uterine lining!
A Complicated History… • 1974 – Albert Yuzpe described the regimen of using ethinylestradiol and norgestrel for emergency contraception • February 14, 1996 – Reproductive Health Technologies Project established a 24 hr emergency contraception hotline number • In the first 5 months of operation, over 25,000 calls were made • February 1997 – FDA publishes notice that certain combined oral contraceptives are approved for off label use as emergency contraceptives • All containing ethinylestradiol + norgestrel or levonorgestrel • Ovral , lo/ovral, nordette, levlen, triphasil, tri-levlen
Initial Progress… • February 1998 – women in Washington state can receive EC from participating pharmacies without a doctors prescription • Eight states have followed: alaska, california, hawaii, maine, massachusetts, new hampshire, new mexico and vermont • September 1998 – FDA approves, Preven, the first dedicated emergency contraception product • Removed from the market in 2004 • July 1999 – FDA approves Plan B, the first progestin-only emergency contraception product • After 1998 WHO study demonstrated that progestin only products are more efficacious and have less side effects
Big Moves for EC… • February 14, 2001 – The Center for Reproductive Rights files a citizens petition with the FDA on behalf of over 70 other medical and public health organizations to make Plan B available OTC • June 2001 – NY Assembly passes legislation requiring hospital ERs to inform rape survivors of EC • Includes catholic institutions • In the following year: Washington state law required hospitals to offer rape victims EC • Many states followed – currently 13 states. NY passed legislation in April 2003
The Politics of Doubt… • April 2003 – Women’s Capitol Corporation submits its application to the FDA for Plan B OTC status • December 2003- FDA advisory committee voted 23 – 4 that plan B be switched to OTC • May 2004 – FDA rejected the OTC switch • Cited concerns about the effects of OTC availability on the sexual behavior of young teenagers • Data at that point had already demonstrated that ready access to Plan B by adolescents as young as 15 did not increase irresponsible sexual behavior • Additional studies more recently consistently demonstrate that women given ready access do not routinely use less effective regular contraception, do not engage more often in high risk sexual behavior, do not become more promiscuous, and do not have increased rates of pregnancy or STDs.
A Sad Day for Science at the FDA… • July 2004 – Barr Laboratories submitted an amended application with age restrictions: OTC for 16 and younger • January 2005 – The FDA fails to meet the deadline • The Center for Reproductive Rights filed a lawsuit against the FDA • September 2005 – the FDA misses its second deadline. • They announced that Plan B was safe for OTC use by women 17 + yrs • but also announced an indefinite delay in reaching a decision. • Requested a 60 day public comment period • Three days later, Susan Wood, the Director of the FDA Office of Women’s Health resigned
“The recent decision announced by the commissioner about emergency contraception, which continues to limit women’s access to a product that would reduce unintended pregnancies and reduce abortions is contrary to my core commitment to improving and advancing women’s health. I have spent the last 15 year working to ensure that science informs good health policy decisions. I can no longer serve as staff when scientific and clinical evidence, fully evaluated and recommended by approval by the professional staff here, has been overruled.” – Susan Wood
At last… • August 2006 – FDA approves OTC sales of Plan B for women/men ages 18 and older • June 2009 – Next Choice, a generic version of plan B, approved for OTC sales for ages 17 and older • July 2009 – Plan B One step approved by the FDA for OTC sales for ages 17 and older
Barriers for our Patients • Pharmaceutical companies are not spending heavily on direct-to-consumer advertising • Only 16 states have enacted legislation requiring hospitals to provide info about and/or initiate emergency contraception therapy to women who have been sexually assaulted • The Department of Justice makes no mention of EC in the National Protocol for Sexual Assault Medical Forensic Examinations • The Department of Defense Pharmacy & Therapeutics Committee removed Plan B from the Basic Core Formulary in May 2002 • Prescription requirement for teens 16 and younger obstructs timely access • OTC availability still limited • Limited by whether a pharmacist has EC or is willing to dispense the EC • 2002 New York study demonstrated that ECs were only available in 50% of pharmacies • Lack of privacy for the patient who has to ask the pharmacist for the drug
Downsides to the OTC status? • Loss of opportunities for physicians to counsel patients • Price increase • Plan B • $35 - 60 • Plan B One Step • $35 - 60 • Next Choice • ~ $40
What Can We Do? • EDUCATE your patients! • A 2009 study in Obstetrics & Gynecology explored Adolescent Comprehension in NYC • 67% of teens aged 12 – 17 yrs had heard of emergency contraception • A 2009 study in JOGNN explored female college students knowledge of EC • 98% heard of EC, but 40% were unsure if EC was the same as RU-486 • 95% knew EC was available in the US, but 33% believed a prescription was required • Only 8% said they received info about EC from their health care provider… • EDUCATE yourself! • A 2009 study in Pediatrics explored emergency contraception knowledge among ER physicians • 43% of the participants were unable to correctly answer 50% of the knowledge based questions • Only 12% identified the correct time period for initiation of EC • Get involved!
References • Von Hertzen H, Piaggio G, Ding J, Chen J, Song S, Bartfai G, Ng E, Gemzell K, Oyunbileg A, Wu S, Cheng W, Ludicke F, Pretnar Am Kirkman R, Mittal S, Khomassuridze A, Apter D, Peregoudow A. Low dose mifepristone and two regumens of levonorgestrel for emergency contraception: a WHO multicentre randomised trial. Lancet 2002;360:1803-10. • Croxatto HB, Ortiz ME, Muller AL. Mechanisms of action of emergency contraception. Steroids 2003;68:1095-8. • Ellertson C, Webb A, Blanchard K, Bigrigg A, HaskellS, Shochet T, Trussell J. Modifying the Yuzperegumen of emergency contraception: a multicenter randomized, controlled trial. ObstetGynecol 2003;101:1160 – 7. • Gold MA, Sucato GS, Conard LA, Hillard PJ. Provision of Emergency Contraception to Adolescents: Position Paper of the Society for Adolescent Medicine. Journal of Adolescent Health 2004;35:66-70. • Klein JD, Barratt MS, Blythe MJ, Diaz A, Rosen DS, Wibbelsman CJ. Emergency Contraception. Pediatrics 2005;116:1038-1047. • Wood AJJ, Drazen JM, Greene MF. A sad day for science at the FDA. N Engl J Med 2005;353:1197-8. • Davidoff F, Trussell J. Plan B and the politics of doubt. J Am Med Assoc 2006;296:1775-8. • Cheng L, Gulmezoglu AM, Piaggo G, Ezcurra E, Van Look PFA. Interventions for emergency contraception. Cochrane Database Syst Rev 2008, Issue 2. • Goyal M, Shao H, Mollen C. Exploring emergency contraception knowledge, prescription practices and barriers to prescritption for adolescents in the emergency department. Pediatrics 2009;123:765-70. • Cremer M, Holland E, Adama B, Klausner D, Nichols S, Ram RS, Alonzo TA. Adolescent Comprehension of Emergency Contraception in New York City. Obstetrics & Gynecology 2009;113:840-844. • Hickey MT. Female College Students’ Knowledge, Perceptions, and Use of Emergency Contraception. JOGNN 2009:38:399-405. • Guttmacher Institute. Facts on American Teen’s Sexual and Reproductive Health. Available at: www.guttmacher.org/pubs/fb_ATSRH.html. Accessed December 5th 2009.