Download
1 / 16
160 likes | 360 Views
QUALITY OF DOCUMENTATION IN MEDICAL RECORDS. NYCHSRO’s Experience in Title I Quality Management Review. New York County Health Services Review Organization Harriet Starr Vice President, Government Contracts. ISSUES IN THE QUALITY OF MEDICAL RECORD DOCUMENTATION.

E N D
QUALITY OF DOCUMENTATION IN MEDICAL RECORDS NYCHSRO’s Experience in Title I Quality Management Review New York County Health Services Review Organization Harriet Starr Vice President, Government Contracts
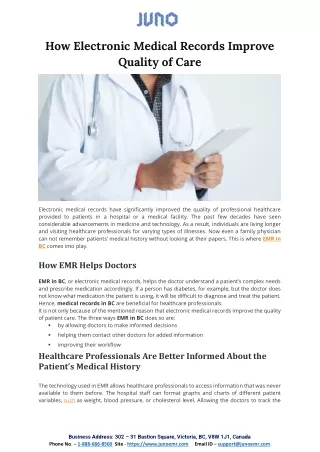
ISSUES IN THE QUALITY OF MEDICAL RECORD DOCUMENTATION • Timely and accurate documentation is associated with: • improved quality of care • seamless continuity of care • enhanced ability to demonstrate equitable delivery of service and improved outcomes • streamlined work processes • reduction in the duplication of work • reliable data sources • increased client, worker and payer satisfaction
ISSUES IN THE QUALITY OF MEDICAL RECORD DOCUMENTATION • Problems with documentation are reflected in lower scores on quality indicators • Quality of care may appear worse than actual
NEW YORK COUNTY HEALTH SERVICES REVIEW ORGANIZATION (NYCHSRO) • Review agent for AIDS Institute Title I Quality Management Program since 2001 • Reviewed the following programs: • Case Management • Treatment Adherence • Food and Nutrition • Home Care • TB DOT • currently reviewing Harm Reduction
NYCHSRO’s EXPERIENCE • Reviewed approximately • 2700 records at 74 programs in 2005 • 2900 records at 44 programs in 2006 • 5600 in last 2 years
NYCHSRO’s EXPERIENCE(continued) • Observations about the quality of documentation in medical records • Based on reviewers’ impressions on completion of a facility’s reviews • Taken mainly from 2005 Food & Nutrition reviews (850 records at 14 providers) and 2006 Case Management review (2700 records at 31 providers) • Findings are representative of 1/3 to 1/2 of records at nearly half of the providers
OBSERVATIONS • Critical information not documented • Lists of community food and nutrition services provided at intake, automatically or on request, but not documented in client record • No documentation for months at a time. Was client disenrolled from program?
OBSERVATIONS • Documentation not dated • Dates of primary care physician visits, lab values (CD4 counts and Viral Loads), and lists of ARV medications missing • PCP appointments discussed in progress notes, but dates of appointments not documented • Photocopies of PCP appointment cards lacked year of service • Progress notes not dated
OBSERVATIONS • Disorganized record • Difficult to locate demographics and follow-up assessments, particularly of client weight and HIV medications • Progress notes not sequential • CD4 and Viral Load values found in different location than dates of these tests
OBSERVATIONS • Incomplete record; documentation stored in too many places • Dates of educational sessions stored in different location than topic • Intake information only kept in oldest of multiple charts
OBSERVATIONS • Incomplete record; documentation stored in too many places (continued) • Primary care data (HIV medications, PCP visits, CD4, viral load) stored only in charts from other programs (e.g., Case Management) and not in Food & Nutrition chart • Demographics only in URS, not in chart
OBSERVATIONS • Documentation is too general • Schedule of educationalsessions provided; no topic available • Topic of educational session identified only as education
OBSERVATIONS • Documentation is too general (continued) • Client need identified as entitlement; no clarification as to whether need was for food stamps, ADAP, Medicaid, etc. • Unable to distinguish between client’s primary medical care and mental health visits
OBSERVATIONS • Documentation is illegible • Illegible handwriting in notes • Can’t identify provider; can’t read signature • Photocopies too light or smeared/distorted • 3rd or 4th copy of multipart form; nothing legible
OBSERVATIONS • Inconsistencies among documentation • Client referred to case manager for assistance with housing, but no documentation that housing status was assessed • Case management assessment and service plan differ as to clients needs. Assessment may indicate “no need identified” in a particular area, but this need addressed in service plan. • Goals for client identified then dropped
OBSERVATIONS • Successful Strategies • Documentation is handled as if third party, unfamiliar with agency, will be reading it • Charts are structured to systematically follow the service delivery and standard of care • Use of forms and flow charts for intake, assessment, primary care indicators • Uniform training and policy for documentation • Electronic medical record – addresses issues of legibility and organization