Download
1 / 52
530 likes | 671 Views
Beyond the EHR. Kevin S.Hughes, MD, FACS Co-Director, Avon Comprehensive Breast Evaluation Center Massachusetts General Hospital Surgeon The Newton-Wellesley Hospital Breast Center. EHR and productivity varies by specialty 100 internists, pediatricians and family practitioners.

E N D
Beyond the EHR Kevin S.Hughes, MD, FACS Co-Director, Avon Comprehensive Breast Evaluation Center Massachusetts General Hospital Surgeon The Newton-Wellesley Hospital Breast Center
EHR and productivity varies by specialty100 internists, pediatricians and family practitioners HemantBhargava, UC Davis Graduate School of Management • Initial implementation • 25 to 33 percent drop in MD productivity • Over time • Internists • Slightly above original productivity • Pediatricians and family practitioners • Remained below original productivity • Explanations • Internists review data entered by others • EMRs more efficient • Pediatricians/family practitioners data entry and documentation • EMR more time-consuming
Quote from a breast surgeon recently on a new EHR • …our productivity is down 28% • Everyone attributes this to the learning curve of xxxx EHR. • I am the highest paid transcriptionist in the state • Each cancer patient chart takes me apprx 1 hour • For the first time in my career, I turned down an add-on patient from one of my outside referrers because I just could not spend one more hour putting a new patient into the computer • I spent 5 hours on Saturday and 4.5 on Sunday catching up on charts from Thurs and Friday and backloading charts of return patients for Tuesday
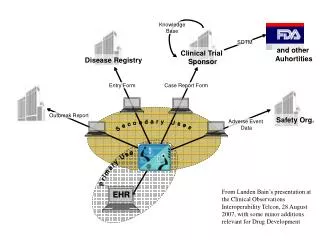
EHR The EHR is a filing cabinet, not a database. The interface is the same for a pediatrician, a neurosurgeon, a cardiologist, and everyone else, as if every specialist wanted data presented the same way. Generic Interface Database Filing Cabinet Or Document Management System
Anesthesia, pathology and breast imaging have set up their own databases and interfaces to deal with their unique needs. They send free text reports into the EHR as the EHR lacks the ability to accept data. EHR Pathology Interface Anesthesia Interface Filing Cabinet Or Document Management System Generic Interface Mammography Interface
HughesRiskAppsBreast Surgery ModuleFree software available at: Kshughes@Partners.org HughesRiskApps.net
Less work + CDS = Higher Quality Patient enters data : Tablet PC iPad Website Patient educational materials Clinical Decision Support Reviews Report & Pedigree Reviews suggested management EHR Clinical Decision Support Documents and Orders
EHR RT Interface Breast Surgery Interface Breast MedOnc Interface
Breast Surgery Module as the prototypeCan be adapted to other disciplines and other cancers easily • Designed to decrease clinician workload • Increase quality by facilitating appropriate course of action • Examples: • Risk algorithms run real-time • Referral letters generated real-time • Improve patient satisfaction • Provide educational materials real-time • Store data needed for certification by NAPBC, ACoS, QOPI, and others • Easily retrieves most data needed for certification with minimal work • Decrease cost • Per above, savings in staff and workload • Decrease in transcription costs of $6000 or more per clinician per year
HughesRiskApps modules follow a simple workflow Existing data Patient data entry Clinical Decision Support (CDS) Printout with suggested actions Clinician editing/enhancing Clinical Decision Support (CDS) Generate orders and documents
Choose how much data you want the patient to enter via the Tablet by choosing the type of survey • Standard • Basic risk information • MGH Standard • Basic risk information plus an extended medical history
Using the HughesRiskApps Tablet questionnaire (With added questions for the Surgery Clinic), a patient can enter her own data • Requiring little or no help from the staff, patients enter their own data. • 5th Grade Reading Level • Available in English, Spanish and Italian Sample screenshots follow
Additional data can be entered by Nurse, Assistant or Clinician
Patient data is downloaded from the LMR (MGH home grown EMR) allowing correlation with patient entered data • Problem List • Medications • Allergies • Procedures Upload of data being developed. Interfaces with other EMRs in development.
Patient data is downloaded from the LMR (MGH home grown EMR) allowing correlation with patient entered data Upload of data being developed. Interfaces with other EMRs in development.
Patient data is downloaded from the LMR (MGH home grown EMR) allowing correlation with patient entered data Upload of data being developed. Interfaces with other EMRs in development.
Patient data is downloaded from the LMR (MGH home grown EMR) allowing correlation with patient entered data Upload of corrected data being developed. Interfaces with other EMRs in development.
Entered by MD (Question set is appropriate to the Chief Complaint)
Entered by MD, but eventually will be an automatic interface with radiology system
Entered by patient via tablet, Clinician/Staff can edit and enhance
Entered by patient via tablet, Clinician/Staff can edit and enhance SubTabs for Risk Factors, Family History (As Table), Pedigree, and Risk Analysis under Tab for specific disease
Entered by patient via tablet, Clinician/Staff can edit and enhance Can view/edit Family History via table or pedigree(See next slide)
Entered by patient via tablet, Clinician/Staff can edit and enhance Can view/edit Family History via pedigree or table (See Prior slide)
Data entered by patient via tablet is used to run risk models
Entered by patient via tablet, Clinician/Staff can edit and enhance
MD enters Physical Exam with interactive breast diagram. Double click on lump to add information
If the Impression includes surgery, Surgical Scheduling screen opens with appropriate procedure pre-chosen. Clinician can edit or change procedure as needed
Orders are pre-filled based on impression and procedures Clinician can add/edit orders
A choice of letters and information sheets are pre-chosen based on orders
Consent, Administrative Paperwork, Patient Education Materials printed
At post operative visits, pathology data is entered and the computer organizes and summaries
Table (Above gray area) shows the procedures and a pathologic summary of the results The more detailed pathology view (Below gray area) relates to the SELECTED procedure
Future timelineWill soon also include Timelines for Breast Imaging, Chemotherapy, RT, and Hormonal Therapy In development Not yet available
Breast Surgery Module as the prototypeCan be adapted to other disciplines that treat breast cancer, as there is significant overlap of data collected
When the final surgery is completed, the cancer summary is derived from the pathology of the individual procedures that had been entered by MD The source of this data can be seen at the procedures tab
After the final surgery, letters are generated to PCP summarizing care, and to Med and Rad Onc, asking for consultation/opinion
Summary of surgery is sent to primary and as part of referral letters to Medical Oncology and Surgical Oncology
Data needed for certification by NAPBC, ACoS, QOPI, and others shown as a report at any time