Download
1 / 20
200 likes | 345 Views
Partners HealthCare Center of Expertise in Academic Healthcare Management. May 14, 2009. Partners Missions. Clinical Care Research Teaching Community Support on Health Issues. How do we generate cash for capital and operating investment?. We Earn it Operations Investment Income

E N D
Partners HealthCareCenter of Expertise in Academic Healthcare Management May 14, 2009
Partners Missions • Clinical Care • Research • Teaching • Community Support on Health Issues
How do we generate cash for capital and operating investment? • We Earn it • Operations • Investment Income • Philanthropy • Debt
Demand for Capital • Since the healthcare industry is very capital intensive one of the biggest challenges we face at Partners is how to balance our capital appetite while ensuring financial stability Capital Investment Access to Debt Financial Stability • To manage this issue, we have developed the Financial Framework
Financial Framework: Key Principles • What is the purpose of the Financial Framework? • Partners uses the Financial Framework as a tool to manage investment and cash flow demands on a system-wide basis, both annually, and on a multi-year basis. The Framework has been reviewed and approved by the Partners Board. • What are the key targets/drivers of the Framework? • Maintain Minimum System-wide Uncommitted Days Cash on hand target of 105 days and a Total Cash target of 200 days . • Uncommitted cash excludes all Board Designated and Sundry Funds and is made up of cash which appears on the Balance Sheet in two lines entitled “Cash & Equivalents” and “Investments” • Achieve System-wide 2% operating margin • Meet required Debt Ratios (Debt Service Coverage: 3.3x and Debt to Cap: <40%)
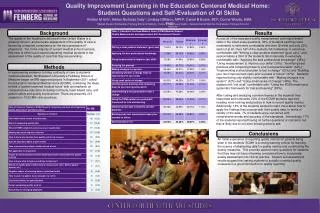
Partners Operating Margins: FY99-FY08 Operating Margin $ in Millions
The Framework • By using the “Financial Framework”, we have provided a platform for internal decision making, which allows senior management to clearly understand what trade-offs must be made to stay within the “envelope”. • From an external perspective, the Rating Agencies, have given Partners high marks for maintaining financial discipline. This structure, in addition to our strong operating performance, has resulted in higher bond ratings for Partners at the same time many of our competitors have seen downgrades. By improving our rating we have been able to borrow money for the benefit of the system at lower rates.
Partners Financial Framework • Operating Margin • Investment Income / Unrealized Gains • Depreciation • Balance Sheet Changes • Principal Payments • Expense/Day Requirement =Net Cash Available for Capital before Philanthropy and Incremental Debt • Philanthropy • Additional Borrowing Capacity = Net Cash Available for Capital - Capital Demand GAP Rationing Process
Financial Framework: Key Elements • Expense/Day Reserves: Reserving for an increase in annual expenses is necessary to maintain the System-wide Uncommitted Days Cash on Hand target of 105 days. • Debt: Partners borrows on behalf of the system. We are currently rated a AA credit by S&P and Moody’s. The Financial Framework is one of the key factors that supports our rating, since it shows a strong management focus on balancing our investment needs, while maintaining our key financial ratios. • Fundraising dollars accrue exclusively to the benefit of the entity/family receiving the gift; they are not available to support System-wide investments.
Partners and Rating Agency Medians What are some of the key ratios that Moody’s and S&P review and how do we compare to the Aa2/AA medians?
How does Partners use the Framework to make decisions? • Margin: Achieving at least a 2% system-wide operating margin is necessary to support the capital needs of the system. • What do we do to meet this objective? • Annual and multi year margin targets are established for each of the Partners families e.g. BWF, MGH, NSMC, NW, PCC as well as all other entities • The ability of each member of Partners HealthCare to maximize their margin is key to the success of this strategy. • Key management actions that may be necessary to achieve these targets are identified. We currently have a major cost management initiative underway.
FY09-FY13 Capital Spending totals $3.2B ($ in Millions)
$540,000 $480,000 $420,000 $360,000 $300,000 $240,000 $180,000 Margin (in $000s) $120,000 $60,000 $0 FY 07 Margin$ ($60,000) FY 08 Margin$ ($120,000) ($180,000) Commercial Other Free Care Mcare Mgd. Medicaid Medicare Total Government Care AMC Total Patient Care Margin Dollars -FY07 vs. FY08 * Excludes BWH DFCI activity
$1.50 FY 2007 FY 2008 $1.25 $1.00 Cents on the Dollar $0.75 $0.50 $0.25 $0.00 Commercial Other Mcare Mgd. Medicaid Medicare Free Care Total Government Care AMC Total Patient Care Cents on the Dollar FY07 vs FY08 * Excludes BWH DFCI activity
Public → Private Payer Cost Shift We estimate that, if the public payers paid at cost, the premium to private employees would be reduced by 16%. In other words, 84% of the premium paid by employers is to cover their own employees and 16% is a hidden tax because government programs do not pay the full cost of the services received.
MY Fundraising: Capital Spending is offset by approximately $200M in Philanthropy proceeds during the FY09-FY13 timeframe FY09-FY13: $208.8M Note: MGH includes $5.3M of Nantucket funds for Facility Renovation; NSMC Fundraising includes current projected fundraising for ACC