Download
1 / 31
310 likes | 435 Views
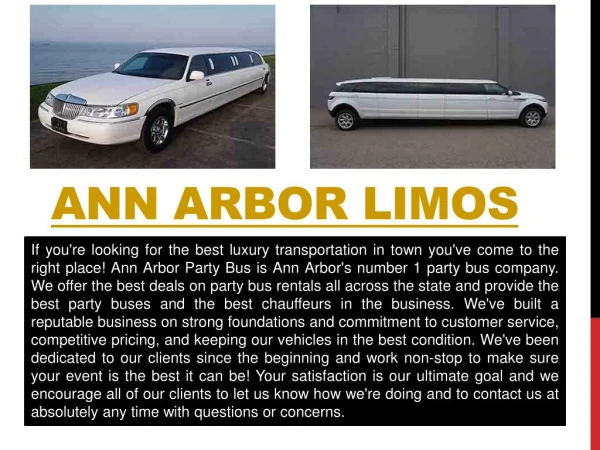
Strategies and Tested Programs to Achieve Optimal Value From Your PBM October 1, 2009 MICUPA Ann Arbor, Michigan. Keith Bruhnsen, MSW Assistant Director, Benefits Office Manager, Prescription Drug Plan. Presentation Topics. Cost Drivers Prescription Drug Trend

E N D
Strategies and Tested Programs to Achieve Optimal Value From Your PBM October 1, 2009 MICUPA Ann Arbor, Michigan Keith Bruhnsen, MSW Assistant Director, Benefits Office Manager, Prescription Drug Plan
Presentation Topics • Cost Drivers • Prescription Drug Trend • U-M Prescription Drug Carve-Out • Plan Design • PBM Selection • Key Strategies • Effective Controls and Innovative Practices • U-M Results • Top Initiatives to Manage Cost /Utilization with you PBM
Drivers of Annual Rx Cost • Utilization creep • Price increases (ingredient cost) • Direct-to-Consumer Advertising – members & physicians • New drug releases and new indications • Blockbuster, Lifestyle and BioTech Drugs • Manufacturer/PBM marketing or switching
Trend Factors 10% 5% 1.7% 3.3% Trend Price Product Utilization = + + • Trend will vary by distribution channels, employer to employer, by region and demographics, by claim processor, and brand vs. generic drugs. • Benefit design, preferred drug list, physician prescribing habits and new, more expensive drugs affect trend and downstream total plan cost.
Projected Trend Ranges for Retail Prescription Drug Carve-Out Coverage 2003-2009
U-M Facts As a Employer: • 34,800 employees & 7000 retiree contracts • 88,000 lives • 7 Unions (25% of actives) • 2008 health care cost $270M (24% Rx) As a Provider: • 4 campus pharmacy’s • 1/2 drug plan scripts written by UM prescribers • Coordinated effort with prescribers & hospital committees
U-M Prescription Drug Carve-out History • Campus task force: studied the problem & proposed solutions • Recommended - Self Insured and self administered rx plan - Consistent coverage and copays - Use internal resources - Create committees and operations - Identify transparent , pass through, PBM partner
U-M Plan Design • Rich plan design, low member out-of-pocket cost • Maintain open formulary of available drugs with standard exclusions (cosmetic, experimental) • Added coverage for psychiatric drugs; oral contraceptives/devices; smoking cessation; $0 co-pay insulin/needles/test strips/lancets, prenatal vitamins; $5,000 fertility lifetime benefit • Mail-order pharmacy (90-day supplies for 2x copay – opened 90-day retail for 3 copays) • Annual Out-of-Pocket max “safety net”: $2,500 individual and $5,000 family • 75% refill limit
2002 PBM Selection 2003 to 2006 Used Traditional PBM Vendor • Merger created disruptive changes • Difficult to accommodate programming request • Deceptive clinical practices, contractual conflicts and service problems • Lack of testing, monitoring claims, and questionable clinical interventions • 2 year rebate audit process
2005 RFP PBM Selection – Phase II Advantages of new vendor (First 4 contractual obligation): • Plan design flexibility • Claims data access • Unbundled services • Improved Pricing • Per transaction basis • 100% pass-through • 100% rebates • Good MAC • Medicare Part-D Employer Subsidy Support • Research opportunities • Innovative partner • Expanded coding
Benefit Office Prescription Drug Plan Functional Areas • Internal Expertise • & Support • Rx Oversight Committee • Rx Advisory Committee (P&T) • College of Pharmacy • Health System Dept • of Pharmacy (340B)
Key Strategies • Manage toward lowest net cost based on evidence based medicine • Adjust plan design to goals, sensitivity to member disruption, and more consumer involvement • Manage rebate game - rebates diminish with generic releases and increased Specialty Rx spending • Future savings are in managing “appropriate use” - utilization, overuse, waste, abuse, and off-label prescribing • Continually educate plan members on plan rationale and individual opportunities
Plan Design Initiatives • Benefit Limitations on Rx Supplies and Quantities • Limits on Fertility, ED, Smoking Cessation and Weight Loss • Plan Exclusions • Standard (cosmetic, anorexiants, etc) • Non-coverage of Rx drugs with OTC alt/equivalents • Use FDA Approved Dosing Limits (maximum daily doses) • Manage Out-of-Network & Compound Claims
Source: Prescription Drug Benefit Cost and Plan Design Report 2008-09 Edition published by Pharmacy Benefit Management Institute, LP, 2008.
Avg. Ingredient Cost Paid Rx/30 Days Supply – Effect of Improved MAC, Statin Switch, and MAC Discount
Research and Other Initiatives • College of Pharmacy • Tablet Splitting Research • Annual Customer Satisfaction Survey • Whitepapers • Switch Programs with UMHHC • Statin • PPI • Nasal Steroid • Diabetes Program • MHealthy: Focus on Medicines
Other U-M Initatives • Specialty Drug Program • Separate vendor • Acquisition plus cost model • Campus Tobacco Intervention Program • No cost for OTC’s • No cost for generic smoking cessation rx products • Reduced cost for 2nd & 3rd Tier rx products • Own Use • Explore GPO for non-profits • Explore contract replenishment model • 340B Pricing Initiatives
Statin Pill-splitting 1-1-08 to 12-31-08 • Results: Safe, No impact on Adherence or Lipid Control • UM 2008: 9944 statin users • 717 unique members pill split, (7.2% of overall statin users) • Free pill splitter annually Impact of Patient Financial Incentives on Participation and Outcomes in a Statin Pill-splitting Program, Choe, et al, AJMC, June 2007
Statin Switch Programs Results 2007-2008 Statins – Brands to Generics • 4777 members lettered • 1900 UM members targeted • 155 users per 1000 • Voluntary switch – both pt and physician must approve • Savings 08 = $208,000, 07 + 08+ Q1/2-2009 = $480,717 • Members saved $65,000 • GDR was 16.81% higher for UM physicians • 4Q2008 GDR = 71% (2Q2009 GDR = 73.9%) • 2007 ROI = 3.66 to 1 Moving From A to Z: Successful Implementation of a Statin Switch Program by a Large Physician Group, American Journal of Managed Care, Fangyan Z. Sy, PharmD; Hae Mi Choe, PharmD; Diane M. Kennedy, BS; Connie J. Standiford, MD; Dawn M. Parsons, RPh, MBA; Keith D. Bruhnsen, MSW; James G. Stevenson, PharmD; and Steven J. Bernstein, MD, MPH, April 2, 2009
UM PPI Switch Program PPI’s – Brands to Generics • July 2007 start-up • 4590 members lettered • 1769 UM members targeted • 83 PPI users per 1000 • 4Q2008 GDR = 65.3%; 2009Q2 = 80.36% • GDR was 12.17% higher for UM physicians • 2008 savings: $163,000, (07+08 =2Q09 = $288,385) • 2007 ROI = 2.29 to 1
2008 UM Program Savings Pill Splitting = $190,370 Statin Switch = $208,000 PPI Switch = $163,000 Nasal Steroids Switch = $ 16,000 Total $575,370 Plus 340B Pricing $891,000
Diabetic Program • Two year study of 2500 diabetics • Reduced co-pays for 4 classes of medications (average $316/yr/pt) • Goal to assess improved adherence • Under further analysis and publication • Transitioned to drug plan A controlled trial of value-based insurance design - The MHealthy: Focus on Diabetes (FOD) trial;Alicen Spaulding , A. Mark Fendrick , William H Herman , James G Stevenson , Dean G Smith , Michael E Chernew , Dawn M Parsons , Keith Bruhnsen and Allison B RosenImplementation Science 2009, 4:19doi:10.1186/1748-5908-4-19, Published: April 7, 2009.
Top Initiatives to Manage Cost/Utilization with Your PBM • Identify Switch Programs • Adopt Dose Optimization • Require Brand Drugs to 3rd Tier Upon Generic Releases • Promote Tablet Splitting • Adopt DAW Penalties • Place FDA Approved Limitations on Dosing with Expensive Products • Identify Prior Authorizations
Top Initiatives – cont. • Evaluate OTC coverage based on plan design and policy • Evaluate Benefit-Based Co-Pay Designs • Evaluate Out of Network and Compound Claim Polices • Review Plan Exclusions (ex – medical foods) • Place Benefit Limitations on Fertility, ED, Smoking Cessation, and Weight Loss • Evaluate if the Medicare Part-D RDS or EGWP is best for your organization • Auditing and plan design testing
Summary • Competing interest in PBM’s profitability & employer cost • Carve-out can control drug spending • Review your plan strategies • Innovative designs can manage use and shape behavior of physicians and members • There are vendors eager to work in a culture of innovation UM Benefits Office: www.umich.edu/~benefits/ Questions: keithb@umich.edu 734 936-1010