Download
1 / 16
160 likes | 599 Views
Selecting the Ventilator and the Mode. Chapter 6. Criteria for Ventilator Selection. Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals can be achieved by using a ventilator?

E N D
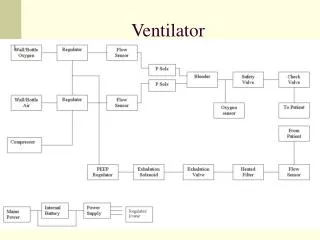
Selecting the Ventilator and the Mode Chapter 6
Criteria for Ventilator Selection • Why does the patient need ventilatory support? • Does the ventilation problem require a special mode? • What therapeutic goals can be achieved by using a ventilator? • Does the patient need to be intubated or can a mask be used? • Will therapeutic intervention take place in an ICU or the patient’s home? • Will ventilatory support be provided for a brief period of time or will long-term assistance be required? • How familiar is the staff with the ventilator under consideration?
Invasive VS Non-invasive • Artificial airway • Translaryngeal airways – oral or nasal endotracheal tubes • Tracheostomy tube • Mask
Advantages of NPPV Avoids complications with artificial airways Provides flexibility in initiating and removing ventilation Reduces requirements for sedation Preserves airway defenses Reduces need for invasive monitoring Disadvantages of NPPV Can cause gastric distention Skin pressure lesions Dry membranes –oral nasal, eye irritations Claustrophobia Poor sleep Noninvasive Ventilation • NPV: negative pressure ventilators • CPAP: continuous positive airway pressure • Used to improve oxygenation • Treat obstructive sleep apnea • NPPV: noninvasive positive pressure ventilation
Invasive Positive Pressure Ventilation • Full ventilatory support: the ventilator provides all the energy necessary to maintain effective alveolar ventilation • Partial ventilatory support: any degree of mechanical ventilation in which the set rates are lower than 6 breaths/min and the patient participates in WOB to help maintain effective alveolar ventilation
Type of breath delivery • Mandatory • Ventilator controls the timing, tidal volume or both • Spontaneous • Patient controls the timing and the tidal volume • Assisted • Characteristics of both spontaneous and mandatory breaths • All or part of the breath is generated by the ventilator • The patient triggers and cycles the breath
Volume Control Volume provided to the patient is constant and independent of what happens to pressure when the patient’s lung characteristics change or when the patient’s effort changes Use when consistent tidal volume delivery is important; goal is to maintain a certain level of PaCO2 Guarantees a specific volume delivery and Ve regardless of changes in lung compliance and resistance Disadvantages: Peak and alveolar pressures rise when lung conditions worsen = alveolar over distention; delivery of flow may be fixed and not match patient demand; inappropriate trigger settings Pressure Control Pressure remains constant whereas volume delivery changes as lung characteristic change Used when the limiting of pressure delivery is important Allows the clinician to set a maximum pressure, reducing the risk of lung over distention, uses a descending flow pattern; may be more comfortable for pts who can breathe spontaneously Disadvantages: volume delivery varies, tidal volume and minute ventilation decrease when lung characteristics deteriorate Control Variables:the independent variable used to establish gas flow to the patient
Modes of Ventilationbreath type and timing of breath delivery • CMV: all breaths are mandatory and can be volume or pressure targeted; breaths can be patient or time triggered • Time triggered breaths in CMV is called control mode • A/C mode is time or patient triggered • Sensitivity settings (pressure or flow)– increased WOB or auto-cycling • Response time: time increment between when a patient effort is detected and when flow from the ventilator to the patient begins • VC-CMC [set Vt, rate, flow to adjust I:E] • PC-CMV (PCV) [set IP, rate, IT to adjust I:E] time cycled
Modes of Ventilationbreath type and timing of breath delivery • IMV / SIMV: periodic volume or pressure targeted breaths occur at set intervals (time triggered), between these mandatory breaths the patient breathes spontaneously at any desired baseline pressure without receiving a mandatory breath • SIMV operates in the same way as IMV except that mandatory breaths are normally patient triggered rather than time triggered; at predetermined intervals the machine waits for the patients next spontaneous effort and then assists the patient by synchronously delivering a mandatory breath • SIMV designed to avoid breath stacking • Spontaneous breaths may be pressure supported • Monitor WOB • Potentially fewer cardiovascular side effects, may be used for weaning
Modes of Ventilationbreath type and timing of breath delivery Spontaneous Modes • Spontaneous breathing • Breathing spontaneously through the ventilator circuit (Brigg’s adaptor, T-piece) • Ventilator monitors the patient’s breathing and can activate alarms • Some ventilators require considerable effort to open inspiratory valves to receive flow • CPAP • Spontaneously breathing through the ventilator circuit • Improving oxygenation in patients with refractory hypoxemia and a low FRC • PSV • Special form of assisted ventilation, always patient triggered
Pressure Support Ventilation • Ventilator provides a constant pressure during inspiration once it sense the patient’s effort • The inspiratory pressure, CPAP, and sensitivity are set, Patient establishes the rate inspiratory flow and inspiratory time • Vt is determined by the pressure gradient, lung characteristics, and patient effort • PSV is used to: • Overcome WOB • Reduce WOB • Provide full ventilatory support in the assist mode (PSmax)
Other Ventilator ModesClosed Loop Ventilation • Bilevel PAP • PRVC • Paug Pressure augmentation, VAPS • MMV • APRV • PAV Familiarize yourself with these (p 96-98).
A patient receives a breath that is patient triggered, pressure targeted and time cycled. What type of breath is it? This is a mandatory, pressure targeted, ventilator cycled breath A patient breathes spontaneously at a baseline pressure of 8cmH2O This is a spontaneous breath, patient triggered and cycled (CPAP) Clinical Rounds 6-1 p. 84What type of breath is it?
Clinical Rounds 6-2 p. 86Volume targeted breaths with Changing Lung Characteristics • What is the approximate inspiratory time? • About 1 sec • What type of waveform is used? • Constant flow waveform, descending ramp (decelerating) • What is the approximate tidal volume delivery for each breath? • Vt = 500ml • What are the peak inspiratory pressures in A B and C? • A = 14cmH2O; B = 25cmH2O; C = 12 cmH2O • What types of lung or thoracic abnormalities can result in reduced compliance? • Pneumonia ARDS pulmonary fibrosis/scarring ascites burns surgical incisions • What would happen to the PIP if compliance went unchanged but airway resistance increased? • PIP increases as more pressure is required to deliver the gas flow Figure 6-1 Graphs for constant flow, volume targeted ventilation; p. 86
Clinical Rounds 6-3 p. 87Pressure targeted breaths with Changing Lung Characteristics • What type of pressure curve is delivered in A, B, and C? • The pressure curve is constant • What type of flow waveform is present during inspiration in A, B, and C? • A descending ramp (decelerating) • Compare the flow-time curve during inspiration in C to that in A. What is the difference between the two? • A drops to zero just at the end of inspiration; C drops to zero before the end of inspiration • Look at the dotted line in C that starts at the flow waveform just when flow drops to zero during inspiration. Look at the volume-time curve (C). What do you notice about this volume-time curve compared to those in A and B? Why is it flat at the top? • The volume curve in C has a short plateau at the top that begins when flow drops to zero during inspiration and ends when exhalation starts. It is flat because the volume is not changing. • Why is volume delivery higher in B than in A? • the lungs in B are more compliant than the lungs in A Figure 6-2 Graphs for pressure targeted Ventilation; p.87
A physician wants to make sure that a patient’s PaCO2 stays at the normal level 50mmHg. Would volume or pressure ventilation best meet this requirement? Volume ventilation should be used since it guarantees volume delivery and minute ventilation. Ventilating pressure can become very high in patients with ARDS. To prevent excessive pressures, what independent variable would be most appropriate, volume or pressure? Pressure targeted ventilation since the goal is to avoid high pressures. Clinical Rounds 6-4 p. 89Pressure or Volume Ventilation