Download
1 / 1
10 likes | 155 Views
Mindfulness based program for infertility (MBPI ): a promising approach in psychosocial care Ana Galhardo *, ** Marina Cunha*,** José Pinto- Gouveia ** anagalhardo@ismt.pt marina_cunha@ismt.pt jpgouveia@fpce.uc.pt

E N D
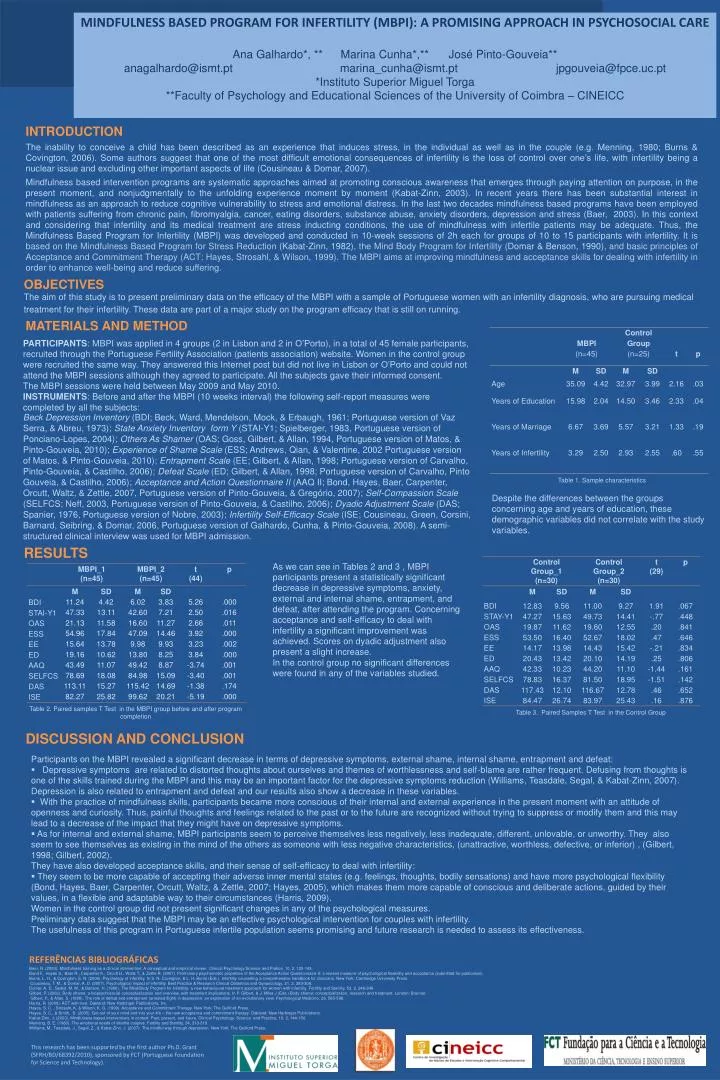
Mindfulness based program for infertility (MBPI): a promising approach in psychosocial care Ana Galhardo*, ** Marina Cunha*,** José Pinto-Gouveia** anagalhardo@ismt.pt marina_cunha@ismt.pt jpgouveia@fpce.uc.pt *Instituto Superior Miguel Torga**Faculty of Psychology and Educational Sciences of the University of Coimbra – CINEICC INTRODUCTION The inability to conceive a child has been described as an experience that induces stress, in the individual as well as in the couple (e.g. Menning, 1980; Burns & Covington, 2006). Some authors suggest that one of the most difficult emotional consequences of infertility is the loss of control over one’s life, with infertility being a nuclear issue and excluding other important aspects of life (Cousineau & Domar, 2007). Mindfulness based intervention programs are systematic approaches aimed at promoting conscious awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding experience moment by moment (Kabat-Zinn, 2003). In recent years there has been substantial interest in mindfulness as an approach to reduce cognitive vulnerability to stress and emotional distress. In the last two decades mindfulness based programs have been employed with patients suffering from chronic pain, fibromyalgia, cancer, eating disorders, substance abuse, anxiety disorders, depression and stress (Baer, 2003). In this context and considering that infertility and its medical treatment are stress inducting conditions, the use of mindfulness with infertile patients may be adequate. Thus, the Mindfulness Based Program for Infertility (MBPI) was developed and conducted in 10-week sessions of 2h each for groups of 10 to 15 participants with infertility. It is based on the Mindfulness Based Program for Stress Reduction (Kabat-Zinn, 1982), the Mind Body Program for Infertility (Domar & Benson, 1990), and basic principles of Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 1999). The MBPI aims at improving mindfulness and acceptance skills for dealing with infertility in order to enhance well-being and reduce suffering. ObjectivES • The aim of this study is to present preliminary data on the efficacy of the MBPI with a sample of Portuguese women with an infertility diagnosis, who are pursuing medical treatment for their infertility. These data are part of a major study on the program efficacy that is still on running. MATERIALS AND METHOD PARTICIPANTS: MBPI was applied in 4 groups (2 in Lisbon and 2 in O’Porto), in a total of 45 female participants, recruited through the Portuguese Fertility Association (patients association) website. Women in the control group were recruited the same way. They answered this Internet post but did not live in Lisbon or O’Porto and could not attend the MBPI sessions although they agreed to participate. All the subjects gave their informed consent. The MBPI sessions were held between May 2009 and May 2010. INSTRUMENTS: Before and after the MBPI (10 weeks interval) the following self-report measures were completed by all the subjects: Beck Depression Inventory (BDI; Beck, Ward, Mendelson, Mock, & Erbaugh, 1961; Portuguese version of Vaz Serra, & Abreu, 1973); State Anxiety Inventoryform Y (STAI-Y1; Spielberger, 1983, Portuguese version of Ponciano-Lopes, 2004); Others As Shamer(OAS; Goss, Gilbert, & Allan, 1994, Portuguese version of Matos, & Pinto-Gouveia, 2010); Experience of Shame Scale (ESS; Andrews, Qian, & Valentine, 2002 Portuguese version of Matos, & Pinto-Gouveia, 2010); Entrapment Scale (EE; Gilbert, & Allan, 1998; Portuguese version of Carvalho, Pinto-Gouveia, & Castilho, 2006); Defeat Scale (ED; Gilbert, & Allan, 1998; Portuguese version of Carvalho, Pinto Gouveia, & Castilho, 2006); Acceptance and Action Questionnaire II (AAQ II; Bond, Hayes, Baer, Carpenter, Orcutt, Waltz, & Zettle, 2007, Portuguese version of Pinto-Gouveia, & Gregório, 2007); Self-Compassion Scale (SELFCS; Neff, 2003, Portuguese version of Pinto-Gouveia, & Castilho, 2006); Dyadic Adjustment Scale (DAS; Spanier, 1976, Portuguese version of Nobre, 2003); Infertility Self-Efficacy Scale (ISE; Cousineau, Green, Corsini, Barnard, Seibring, & Domar, 2006, Portuguese version of Galhardo, Cunha, & Pinto-Gouveia, 2008). A semi-structured clinical interview was used for MBPI admission. • Table 1. Sample characteristics Despite the differences between the groups concerning age and years of education, these demographic variables did not correlate with the study variables. RESULTS As we can see in Tables 2 and 3 , MBPI participants present a statistically significant decrease in depressive symptoms, anxiety, external and internal shame, entrapment, and defeat, after attending the program. Concerning acceptance and self-efficacy to deal with infertility a significant improvement was achieved. Scores on dyadic adjustment also present a slight increase. In the control group no significant differences were found in any of the variables studied. Table 2. Paired samples T Test in the MBPI group before and after program completion Table 3. Paired Samples T Test in the Control Group DISCUSSION AND CONCLUSION • Participants on the MBPI revealed a significant decrease in terms of depressive symptoms, external shame, internal shame, entrapment and defeat: • Depressive symptoms are related to distorted thoughts about ourselves and themes of worthlessness and self-blame are rather frequent. Defusing from thoughts is one of the skills trained during the MBPI and this may be an important factor for the depressive symptoms reduction (Williams, Teasdale, Segal, & Kabat-Zinn, 2007). Depression is also related to entrapment and defeat and our results also show a decrease in these variables. • With the practice of mindfulness skills, participants became more conscious of their internal and external experience in the present moment with an attitude of openness and curiosity. Thus, painful thoughts and feelings related to the past or to the future are recognized without trying to suppress or modify them and this may lead to a decrease of the impact that they might have on depressive symptoms. • As for internal and external shame, MBPI participants seem to perceive themselves less negatively, less inadequate, different, unlovable, or unworthy. They also seem to see themselves as existing in the mind of the others as someone with less negative characteristics, (unattractive, worthless, defective, or inferior) , (Gilbert, 1998; Gilbert, 2002). • They have also developed acceptance skills, and their sense of self-efficacy to deal with infertility: • They seem to be more capable of accepting their adverse inner mental states (e.g. feelings, thoughts, bodily sensations) and have more psychological flexibility (Bond, Hayes, Baer, Carpenter, Orcutt, Waltz, & Zettle, 2007; Hayes, 2005), which makes them more capable of conscious and deliberate actions, guided by their values, in a flexible and adaptable way to their circumstances (Harris, 2009). • Women in the control group did not present significant changes in any of the psychological measures. • Preliminary data suggest that the MBPI may be an effective psychological intervention for couples with infertility. • The usefulness of this program in Portuguese infertile population seems promising and future research is needed to assess its effectiveness. REFERÊNCIAS BIBLIOGRÁFICAS Baer, R. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology:Science and Pratice, 10, 2, 125-143. Bond F., Hayes S., Baer R., Carpenter K., Orcutt H., Waltz T., & Zettle R. (2007). Preliminary psychometric properties of the Acceptance Action Questionnaire-II: a revised measure of psychological flexibility and acceptance (submitted for publication). Burns, L. H., & Covington, S. N. (2006). Psychology of infertility. In S. N. Covington, & L. H. Burns (Eds.). Infertility counseling a comprehensive handbook for clinicians. New York: Cambridge University Press. Cousineau, T. M., & Domar, A. D. (2007). Psychological impact of infertility. Best Practice & Research Clinical Obstetrics and Gynaecology, 21, 2, 293-308. Domar, A. D., Seibel, M. M., & Benson, H. (1990). The Mind/Body Program for Infertility: a new behavioural treatment approach for women with infertility. Fertility and Sterility, 53, 2, 246-249. Gilbert, P. (2002). Body shame: a biopsychosocial conceptualization and overview, with treatment implications. In P. Gilbert, & J. Miles J (Eds.) Body shame: conceptualization, research and treatment. London: Brunner. Gilbert, P., & Allan, S. (1998). The role of defeat and entrapment (arrested flight) in depression: an exploration of an evolutionary view. Psychological Medicine, 28, 585-598. Harris, R. (2009). ACT with love. Oakland: New Harbinger Publications, Inc. Hayes, S. C. , Strosahl, K, & Wilson, K. G. (1999). Acceptance and Commitment Therapy. New York: The Guilford Press. Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life – the new acceptance and commitment therapy. Oakland: New Harbinger Publications. Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10, 2, 144-156. Menning, B. E. (1980). The emotional needs of infertile couples. Fertility and Sterility, 34, 313-319. Williams, M., Teasdale, J., Segal, Z., & Kabat-Zinn, J. (2007). The mindful way through depression. New York: The Guilford Press. This research has been supported by the first author Ph.D. Grant (SFRH/BD/68392/2010), sponsored by FCT (Portuguese Foundation for Science and Technology).