Download
1 / 1
10 likes | 112 Views
No. 106. Management of renal masses in transplant allografts at an Australian Kidney-Pancreas transplant u nit. Michael Su, Nicholas Campbell, Howard Lau Department of Urology, Westmead Hospital, Sydney, Australia. Posters Proudly Supported by:. Results. Introduction

E N D
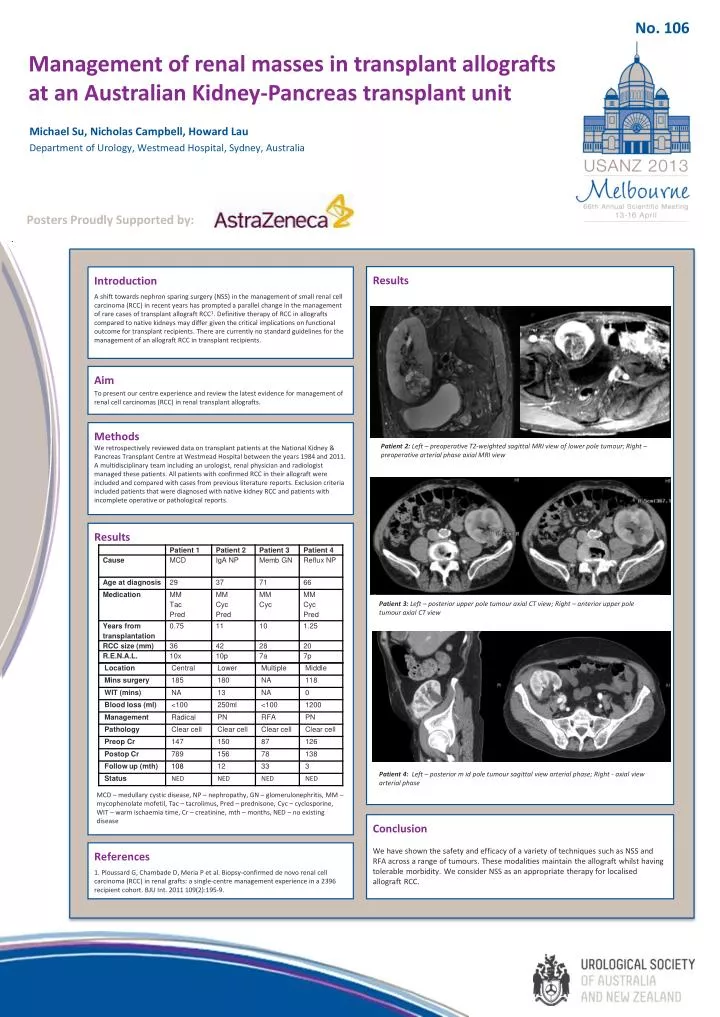
No. 106 Management of renal masses in transplant allografts at an Australian Kidney-Pancreas transplant unit Michael Su, Nicholas Campbell, Howard Lau Department of Urology, Westmead Hospital, Sydney, Australia Posters Proudly Supported by: Results Introduction A shift towards nephron sparing surgery (NSS) in the management of small renal cell carcinoma (RCC) in recent years has prompted a parallel change in the management of rare cases of transplant allograft RCC1. Definitive therapy of RCC in allografts compared to native kidneys may differ given the critical implications on functional outcome for transplant recipients. There are currently no standard guidelines for the management of an allograft RCC in transplant recipients. • Aim • To present our centre experience and review the latest evidence for management of renal cell carcinomas (RCC) in renal transplant allografts. Methods We retrospectively reviewed data on transplant patients at the National Kidney & Pancreas Transplant Centre at Westmead Hospital between the years 1984 and 2011. A multidisciplinary team including an urologist, renal physician and radiologist managed these patients. All patients with confirmed RCC in their allograft were included and compared with cases from previous literature reports. Exclusion criteria included patients that were diagnosed with native kidney RCC and patients with incomplete operative or pathological reports. Patient 2: Left – preoperative T2-weighted sagittal MRI view of lower pole tumour; Right – preoperative arterial phase axial MRI view Results Patient 3: Left – posterior upper pole tumour axial CT view; Right – anterior upper pole tumour axial CT view Patient 4: Left – posterior m id pole tumour sagittal view arterial phase; Right - axial view arterial phase MCD – medullary cystic disease, NP – nephropathy, GN – glomerulonephritis, MM – mycophenolatemofetil, Tac – tacrolimus, Pred – prednisone, Cyc – cyclosporine, WIT – warm ischaemia time, Cr – creatinine, mth – months, NED – no existing disease Conclusion We have shown the safety and efficacy of a variety of techniques such as NSS and RFA across a range of tumours. These modalities maintain the allograft whilst having tolerable morbidity. We consider NSS as an appropriate therapy for localised allograft RCC. References 1. Ploussard G, Chambade D, Meria P et al. Biopsy-confirmed de novo renal cell carcinoma (RCC) in renal grafts: a single-centre management experience in a 2396 recipient cohort. BJU Int. 2011 109(2):195-9.






