Download
1 / 1
10 likes | 142 Views
Can Direct Aperture Optimized IMRT using only Conventional Jaws produce satisfactory treatment plans for Head and Neck C ancer?. Guangwei Mu, Ping Xia Department of Radiation Oncology, University of California San Francisco, San Francisco, CA, USA. INTRODUCTION. RESULTS. Background:

E N D
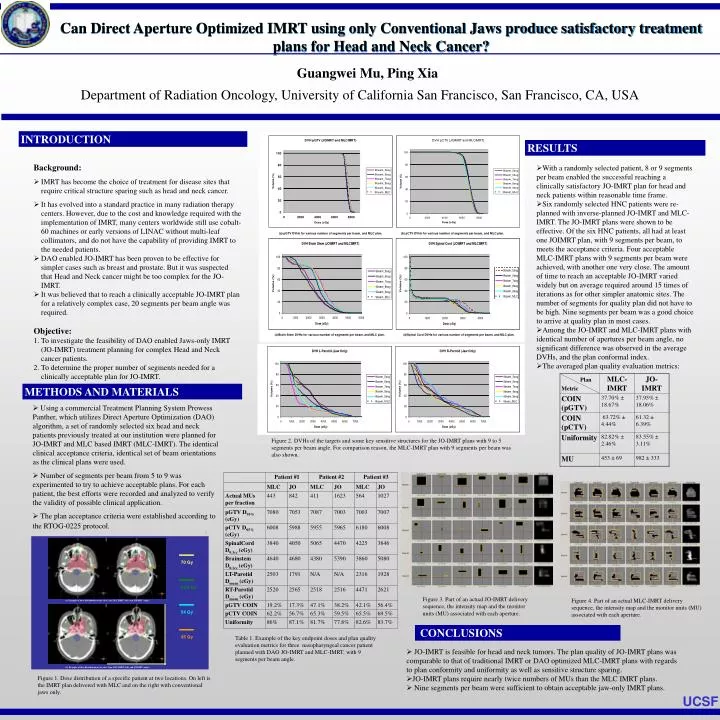
Can Direct Aperture Optimized IMRT using only Conventional Jaws produce satisfactory treatment plans for Head and NeckCancer? Guangwei Mu, Ping Xia Department of Radiation Oncology, University of California San Francisco, San Francisco, CA, USA INTRODUCTION RESULTS Background: • IMRT has become the choice of treatment for disease sites that require critical structure sparing such as head and neck cancer. • It has evolved into a standard practice in many radiation therapy centers. However, due to the cost and knowledge required with the implementation of IMRT, many centers worldwide still use cobalt-60 machines or early versions of LINAC without multi-leaf collimators, and do not have the capability of providing IMRT to the needed patients. • DAO enabled JO-IMRT has been proven to be effective for simpler cases such as breast and prostate. But it was suspected that Head and Neck cancer might be too complex for the JO-IMRT. • It was believed that to reach a clinically acceptable JO-IMRT plan for a relatively complex case, 20 segments per beam angle was required. Objective: • To investigate the feasibility of DAO enabled Jaws-only IMRT (JO-IMRT) treatment planning for complex Head and Neck cancer patients. • To determine the proper number of segments needed for a clinically acceptable plan for JO-IMRT. • With a randomly selected patient, 8 or 9 segments per beam enabled the successful reaching a clinically satisfactory JO-IMRT plan for head and neck patients within reasonable time frame. • Six randomly selected HNC patients were re-planned with inverse-planned JO-IMRT and MLC-IMRT. The JO-IMRT plans were shown to be effective. Of the six HNC patients, all had at least one JOIMRT plan, with 9 segments per beam, to meets the acceptance criteria. Four acceptable MLC-IMRT plans with 9 segments per beam were achieved, with another one very close. The amount of time to reach an acceptable JO-IMRT varied widely but on average required around 15 times of iterations as for other simpler anatomic sites. The number of segments for quality plan did not have to be high. Nine segments per beam was a good choice to arrive at quality plan in most cases. • Among the JO-IMRT and MLC-IMRT plans with identical number of apertures per beam angle, no significant difference was observed in theaverage DVHs, and the plan conformal index. • The averaged plan quality evaluation metrics: METHODS AND MATERIALS • Using a commercial Treatment Planning System Prowess Panther, which utilizes Direct Aperture Optimization (DAO) algorithm, a set of randomly selected six head and neck patients previously treated at our institution were planned for JO-IMRT and MLC based IMRT (MLC-IMRT). The identical clinical acceptance criteria, identical set of beam orientations as the clinical plans were used. • Number of segments per beam from 5 to 9 was experimented to try to achieve acceptable plans. For each patient, the best efforts were recorded and analyzed to verify the validity of possible clinical application. • The plan acceptance criteria were established according to the RTOG-0225 protocol. Figure 2. DVHs of the targets and some key sensitive structures for the JO-IMRT plans with 9 to 5 segments per beam angle. For comparison reason, the MLC-IMRT plan with 9 segments per beam was also shown. Figure 3. Part of an actual JO-IMRT delivery sequence, the intensity map and the monitor units (MU) associated with each aperture. Figure 4. Part of an actual MLC-IMRT delivery sequence, the intensity map and the monitor units (MU) associated with each aperture. CONCLUSIONS Table 1. Example of the key endpoint doses and plan quality evaluation metrics for three nasopharyngeal cancer patient planned with DAO JO-IMRT and MLC-IMRT, with 9 segments per beam angle. JO-IMRT is feasible for head and neck tumors. The plan quality of JO-IMRT plans was comparable to that of traditional IMRT or DAO optimized MLC-IMRT plans with regards to plan conformity and uniformity as well as sensitive structure sparing. JO-IMRT plans require nearly twice numbers of MUs than the MLC IMRT plans. Nine segments per beam weresufficient to obtain acceptable jaw-only IMRT plans. Figure 1. Dose distribution of a specific patient at two locations. On left is the IMRT plan delivered with MLC and on the right with conventional jaws only. UCSF .