Download
1 / 1
10 likes | 92 Views
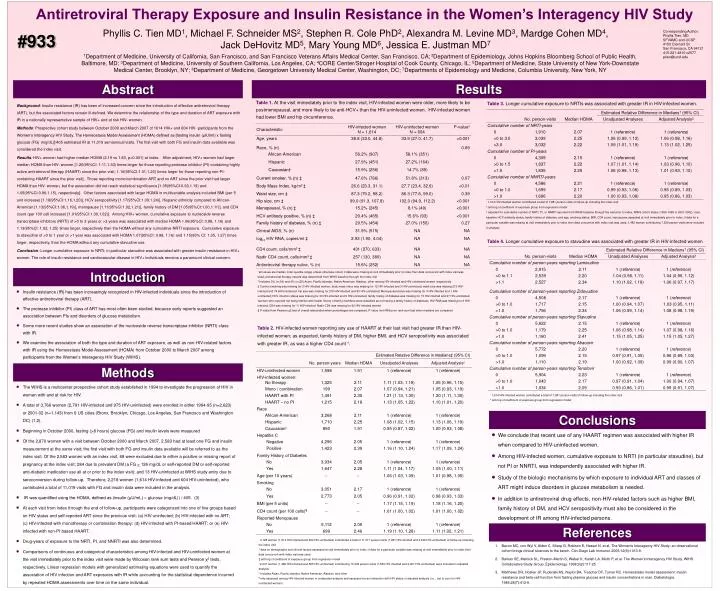
Antiretroviral Therapy Exposure and Insulin Resistance in the Women’s Interagency HIV Study. Phyllis C. Tien MD 1 , Michael F. Schneider MS 2 , Stephen R. Cole PhD 2 , Alexandra M. Levine MD 3 , Mardge Cohen MD 4 , Jack DeHovitz MD 5 , Mary Young MD 6 , Jessica E. Justman MD 7.

E N D
Antiretroviral Therapy Exposure and Insulin Resistance in the Women’s Interagency HIV Study Phyllis C. Tien MD1, Michael F. Schneider MS2, Stephen R. Cole PhD2, Alexandra M. Levine MD3, Mardge Cohen MD4, Jack DeHovitz MD5, Mary Young MD6, Jessica E. Justman MD7 Corresponding Author: Phyllis Tien, MD SFVAMC and UCSF 4150 Clement St San Francisco, CA 94121 415-221-4810 x2577 ptien@ucsf.edu #933 1Department of Medicine, University of California, San Francisco, and San Francisco Veterans Affairs Medical Center, San Francisco, CA; 2Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD; 3Department of Medicine, University of Southern California, Los Angeles, CA; 4CORE Center/Stroger Hospital of Cook County, Chicago, IL; 5Department of Medicine, State University of New York-Downstate Medical Center, Brooklyn, NY; 6Department of Medicine, Georgetown University Medical Center, Washington, DC; 7Departments of Epidemiology and Medicine, Columbia University, New York, NY Results Abstract Table 1.At the visit immediately prior to the index visit, HIV-infected women were older, more likely to be postmenopausal, and more likely to be anti-HCV+ than the HIV-uninfected women. HIV-infected women had lower BMI and hip circumference. Table 3. Longer cumulative exposure to NRTIs was associated with greater IR in HIV-infected women. Background: Insulin resistance (IR) has been of increased concern since the introduction of effective antiretroviral therapy (ART), but the associated factors remain ill-defined. We determine the relationship of the type and duration of ART exposure with IR in a nationally representative sample of HIV+ and at risk HIV- women. Methods: Prospective cohort study between October 2000 and March 2007 of 1614 HIV+ and 604 HIV- participants from the Women’s Interagency HIV Study. The Homeostasis Model Assessment (HOMA) defined as [fasting insulin (µIU/ml) x fasting glucose (FG) (mg/dL)]/405 estimated IR at 11,019 semiannual visits. The first visit with both FG and insulin data available was considered the index visit. Results: HIV+ women had higher median HOMA (2.19 vs 1.83, p<0.001) at index. After adjustment, HIV+ women had larger median HOMA than HIV- women [1.20(95%CI: 1.11,1.30) times larger for those reporting protease inhibitor (PI)-containing highly active antiretroviral therapy (HAART) since the prior visit; 1.10(95%CI:1.01,1.20) times larger for those reporting non-PI-containing HAART since the prior visit]. Those reporting mono/combination ART and no ART since the prior visit had larger HOMA than HIV- women, but the association did not reach statistical significance [1.05(95%CI:0.93,1.19) and 1.05(95%CI:0.96,1.15), respectively]. Other factors associated with larger HOMA in multivariable analysis included BMI (per 5 unit increase) [1.18(95%CI:1.16,1.20)], HCV seropositivity [1.17(95%CI:1.09,1.24)], Hispanic ethnicity compared to African-American [1.13(95%CI:1.06,1.19)], menopause [1.11(95%CI:1.02,1.21)], family history of DM [1.05(95%CI:1.00,1.11)], and CD4 count (per 100 cell increase) [1.01(95%CI:1.00,1.02)]. Among HIV+ women, cumulative exposure to nucleoside reverse transcriptase inhibitors (NRTI) of >0 to 3 years or >3 years was associated with median HOMA 1.06(95%CI: 0.98, 1.16) and 1.13(95%CI: 1.02, 1.25) times larger, respectively than the HOMA without any cumulative NRTI exposure. Cumulative exposure to stavudine of >0 to 1 year or >1 year was associated with HOMA 1.07(95%CI: 0.98, 1.16) and 1.15(95% CI: 1.05, 1.27) times larger, respectively, than the HOMA without any cumulative stavudine use. Conclusion: Longer cumulative exposure to NRTI; in particular stavudine was associated with greater insulin resistance in HIV+ women. The role of insulin resistance and cardiovascular disease in HIV+ individuals remains a paramount clinical concern. * 1,614 HIV-infected women contributed a total of 7,981 person-visits of follow-up including the index visit † anti-log of coefficient of exposure group from regression model ‡ adjusted for cumulative number of NRTI, PI, or NNRTI reported from WIHS baseline through the visit prior to index, WIHS cohort status (1994-1995 or 2001-2002), race, baseline HCV antibody status, family history of diabetes, and age, smoking status, BMI, CD4 count, menopause assessed at visit immediately prior to index; if data for a particular variable was missing at visit immediately prior to index then data concurrent with index visit was used; 1,482 women contributing 7,529 person-visits were included in analysis Table 4. Longer cumulative exposure to stavudine was associated with greater IR in HIV-infected women Introduction * all values are median (inter-quartile range) unless otherwise noted; if data were missing at visit immediately prior to index then data concurrent with index visit was used; antiretroviral therapy naiveté was determined from WIHS baseline through the index visit † Includes 3% (n=54) and 4% (n=25) Asian, Pacific Islander, Native American, Alaskan, other among HIV-infected and HIV-uninfected women respectively ‡ Current smoking was missing for 3 HIV-infected women; body mass index was missing for 12 HIV-infected and 3 HIV-uninfected; waist size was missing 215 HIV-infected and 79 HIV-uninfected; hip size was missing for 216 HIV-infected and 80 HIV-uninfected; Menopausal status was missing for 4 HIV-infected and 1 HIV-uninfected; HCV infection status was missing for 33 HIV-infected and 9 HIV-uninfected; family history of diabetes was missing for 73 HIV-infected and 27 HIV-uninfected (women who reported not being familiar with health history of family members were classified as not having a family history of diabetes); HIV RNA was missing for 6 HIV-infected; CD4 was missing for 11 HIV-infected; Nadir CD4 was missing for 92 HIV-infected women § P-value from Pearson χ2 test of overall association when percentages are compared, P-value from Wilcoxon rank sum test when medians are compared • Insulin resistance (IR) has been increasingly recognized in HIV-infected individuals since the introduction of effective antiretroviral therapy (ART). • The protease inhibitor (PI) class of ART has most often been studied, because early reports suggested an association between PIs and disorders of glucose metabolism. • Some more recent studies show an association of the nucleoside reverse transcriptase inhibitor (NRTI) class with IR. • We examine the association of both the type and duration of ART exposure, as well as non-HIV-related factors with IR using the Homeostasis Model Assessment (HOMA) from October 2000 to March 2007 among participants from the Women’s Interagency HIV Study (WIHS). Table 2. HIV-infected women reporting any use of HAART at their last visit had greater IR than HIV-infected women; as expected, family history of DM, higher BMI, and HCV seropositivity was associated with greater IR, as was a higher CD4 count†. Methods • The WIHS is a multicenter prospective cohort study established in 1994 to investigate the progression of HIV in women with and at risk for HIV. • A total of 3,766 women (2,791 HIV-infected and 975 HIV-uninfected) were enrolled in either 1994-95 (n=2,623) or 2001-02 (n=1,143) from 6 US cities (Bronx, Brooklyn, Chicago, Los Angeles, San Francisco and Washington DC) (1,2). • Beginning in October 2000, fasting (>8 hours) glucose (FG) and insulin levels were measured • Of the 2,870 women with a visit between October 2000 and March 2007, 2,583 had at least one FG and insulin measurement at the same visit; the first visit with both FG and insulin data available will be referred to as the index visit. Of the 2,583 women with an index visit, 68 were excluded due to either a positive or missing report of pregnancy at the index visit; 284 due to prevalent DM (a FG > 126 mg/dL or self-reported DM or self-reported anti-diabetic medication use all at or prior to the index visit); and 13 HIV-uninfected at WIHS study entry due to seroconversion during follow-up. Therefore, 2,218 women (1,614 HIV-infected and 604 HIV-uninfected), who contributed a total of 11,019 visits with FG and insulin data were included in the analysis. • IR was quantified using the HOMA, defined as (insulin (μU/mL) glucose (mg/dL)) / 405. (3) • At each visit from index through the end of follow-up, participants were categorized into one of five groups based on HIV status and self-reported ART since the previous visit: (a) HIV-uninfected; (b) HIV-infected with no ART; (c) HIV-infected with monotherapy or combination therapy; (d) HIV-infected with PI-based HAART; or (e) HIV-infected with non-PI based HAART. • Drug-years of exposure to the NRTI, PI, and NNRTI was also determined. • Comparisons of continuous and categorical characteristics among HIV-infected and HIV-uninfected women at the visit immediately prior to the index visit were made by Wilcoxon rank sum tests and Pearson χ2 tests, respectively. Linear regression models with generalized estimating equations were used to quantify the association of HIV infection and ART exposures with IR while accounting for the statistical dependence incurred by repeated HOMA assessments over time on the same individual. * 1,614 HIV-infected women contributed a total of 7,981 person-visits of follow-up including the index visit † anti-log of coefficient of exposure group from regression model Conclusions • We conclude that recent use of any HAART regimen was associated with higher IR when compared to HIV-uninfected women. • Among HIV-infected women, cumulative exposure to NRTI (in particular stavudine), but not PI or NNRTI, was independently associated with higher IR. • Study of the biologic mechanisms by which exposure to individual ART and classes of ART might induce disorders in glucose metabolism is needed. • In addition to antiretroviral drug effects, non-HIV-related factors such as higher BMI, family history of DM, and HCV seropositivity must also be considered in the development of IR among HIV-infected persons. References * 2,128 women (1,614 HIV-infected and 604 HIV-uninfected) contributed a total of 11,017 person-visits (7,981 HIV-infected and 3,036 HIV-uninfected) of follow-up including the index visit † data on demographic and clinical factors assessed at visit immediately prior to index; if data for a particular variable was missing at visit immediately prior to index then data concurrent with index visit was used ‡ anti-log of coefficient of exposure group from regression model § 2,047 women (1,482 HIV-infected and 565 HIV-uninfected) contributing 10,436 person-visits (7,529 HIV-infected and 2,907 HIV-uninfected) were included in adjusted analysis || Includes Asian, Pacific Islander, Native American, Alaskan, and other ¶ only assessed among HIV-infected women in unadjusted analysis and assessed via an interaction with HIV status in adjusted analysis (i.e., set to zero for HIV-uninfected women) 1. Bacon MC, von Wyl V, Alden C, Sharp G, Robison E, Hessol N, et al. The Women's Interagency HIV Study: an observational cohort brings clinical sciences to the bench. Clin Diagn Lab Immunol. 2005;12(9):1013-9. 2. Barkan SE, Melnick SL, Preston-Martin S, Weber K, Kalish LA, Miotti P, et al. The Women's Interagency HIV Study. WIHS Collaborative Study Group. Epidemiology. 1998;9(2):117-25. 3. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412-9.