Download
1 / 1
10 likes | 136 Views
Features of Epstein-Barr Virus (EBV) reactivation after reduced intensity conditioning (RIC) allogeneic stem cell transplantation (allo-SCT).

E N D
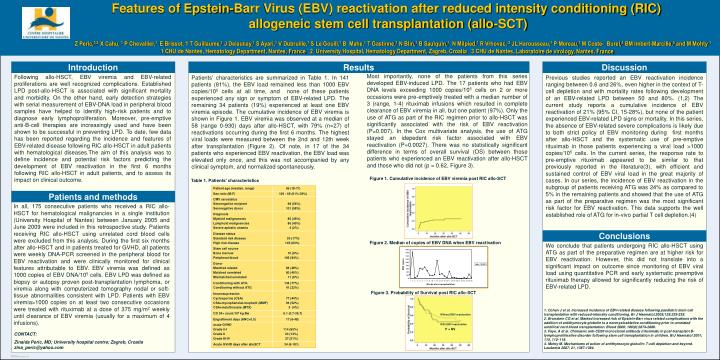
Features of Epstein-Barr Virus (EBV) reactivation after reduced intensity conditioning (RIC) allogeneic stem cell transplantation (allo-SCT) ZPeric,1,2 X Cahu, 1PChevallier,1 E Brissot, 1 T Guillaume,1 JDelaunay,1 S Ayari,1 VDubruille,1 SLe Gouill,1 B Mahe,1 T Gastinne,1 N Blin,1 BSaulquin,1NMilpied,1R Vrhovac,2JL Harousseau,1P Moreau,1 MCoste-Burel,3 BMImbert-Marcille,3 and M Mohty1 1 CHU de Nantes, Hematology Department, Nantes, France2 University Hospital, Hematology Department, Zagreb, Croatia3 CHU de Nantes, Laboratoire de virology, Nantes, France Introduction Results Results 2 Discussion Patients' characteristics are summarized in Table 1. In 141 patients (81%), the EBV load remained less than 1000 EBV copies/105 cells at all time, and none of these patients experienced any sign or symptom of EBV-related LPD. The remaining 34 patients (19%) experienced at least one EBV viremia episode. The cumulative incidence of EBV viremia is shown in Figure 1. EBV viremia was observed at a median of 58 (range 0-930) days after allo-HSCT, with 79% (n=27) of reactivations occurring during the first 6 months. The highest viral loads were measured between the 2nd and 12th week after transplantation (Figure 2). Of note, in 17 of the 34 patients who experienced EBV reactivation, the EBV load was elevated only once, and this was not accompanied by any clinical symptom, and normalized spontaneously. Previous studies reported an EBV reactivation incidence ranging between 0.6 and 26%, even higher in the context of T-cell depletion and with mortality rates following development of an EBV-related LPD between 50 and 80%. (1,2) The current study reports a cumulative incidence of EBV reactivation of 21% (95% CI, 15-28%), but none of the patient experienced EBV-related LPD signs or mortality. In this series, the absence of EBV-related severe complications is likely due to both strict policy of EBV monitoring during first months after allo-HSCT and the systematic use of pre-emptive rituximab in those patients experiencing a viral load >1000 copies/105 cells. In the current series, the response rate to pre-emptive rituximab appeared to be similar to that previously reported in the literature(3), with efficient and sustained control of EBV viral load in the great majority of cases. In our series, the incidence of EBV reactivation in the subgroup of patients receiving ATG was 24% as compared to 5% in the remaining patients and showed that the use of ATG as part of the preparative regimen was the most significant risk factor for EBV reactivation. This data supports the well established role of ATG for in-vivo partial T cell depletion.(4) Most importantly, none of the patients from this series developed EBV-induced LPD. The 17 patients who had EBV DNA levels exceeding 1000 copies/105 cells on 2 or more occasions were pre-emptively treated with a median number of 3 (range, 1-4) rituximab infusions which resulted in complete clearance of EBV viremia in all, but one patient (97%). Only the use of ATG as part of the RIC regimen prior to allo-HSCT was significantly associated with the risk of EBV reactivation (P=0.007). In theCox multivariate analysis, the use of ATG stayed anidepedent risk factor associated with EBV reactivation (P=0.0027). There was no statistically significant difference in terms of overall survival (OS) between those patients who experienced an EBV reactivation after allo-HSCT and those who did not (p = 0.62, Figure 3). Following allo-HSCT, EBV viremia and EBV-related proliferations are well recognized complications. Established LPD post-allo-HSCT is associated with significant mortality and morbidity. On the other hand, early detection strategies with serial measurement of EBV-DNA load in peripheral blood samples have helped to identify high-risk patients and to diagnose early lymphoproliferation. Moreover, pre-emptive anti-B-cell therapies are increasingly used and have been shown to be successful in preventing LPD. To date, few data has been reported regarding the incidence and features of EBV-related disease following RIC allo-HSCT in adult patients with hematological diseases.The aim of this analysis was to define incidence and potential risk factors predicting the development of EBV reactivation in the first 6 months following RIC allo-HSCT in adult patients, and to assess its impact on clinical outcome. Figure 1. Cumulative incidence of EBV viremia post RIC allo-SCT Table 1. Patients’ characteristics Patients and methods In all, 175 consecutive patients who received a RIC allo-HSCT for hematological malignancies in a single institution (University Hospital of Nantes) between January 2005 and June 2009 were included in this retrospective study. Patients receiving RIC allo-HSCT using unrelated cord blood cells were excluded from this analysis. During the first six months after allo-HSCT and in patients treated for GVHD, all patients were weekly DNA-PCR screened in the peripheral blood for EBV reactivation and were clinically monitored for clinical features attributable to EBV. EBV viremia was defined as 1000 copies of EBV DNA/105 cells. EBV LPD was defined as biopsy or autopsy proven post-transplantation lymphoma, or viremia along with computerized tomography nodal or soft-tissue abnormalities consistent with LPD. Patients with EBV viremia>1000 copies on at least two consecutive occasions were treated with rituximab at a dose of 375 mg/m2 weekly until clearance of EBV viremia (usually for a maximum of 4 infusions). Conclusions We conclude that patients undergoing RIC allo-HSCT using ATG as part of the preparative regimen are at higher risk for EBV reactivation. However, this did not translate into a significant impact on outcome since monitoring of EBV viral load using quantitative PCR and early systematic preemptive rituximab therapy allowed for significantly reducing the risk of EBV-related LPD. Figure 2. Median of copies of EBV DNA when EBV reactivation Figure 3. Probability of Survival post RIC allo-SCT 1. Cohen Jet al. Increased incidence of EBV-related disease following paediatric stem cell transplantation with reduced-intensity conditioning. Br J Haematol.2005;129:229-239. 2. Brunstein CGet al. Marked increased risk of Epstein-Barr virus relatedcomplications with the addition of antithymocyte globulin to a nonmyeloablative conditioning prior to unrelated umbilical cord blood transplantation. Blood 2006; 108(8):2874-2880. 3. Faye, A et al. Chimaeric anti-CD20 monoclonal antibody (rituximab) in post-transplant B-lymphoproliferative disorder followingstem cell transplantation in children. BrJ Haematol 2001; 115, 112–118. 4. Mohty M. Mechanisms of action of antithymocyte globulin: T-cell depletion and beyond. Leukemia 2007; 21, 1387-1394. Without EBV reactivation With EBV reactivation P = NS CONTACT: Zinaida Peric, MD; University hospital centre; Zagreb, Croatia zina_peric@yahoo.com