Download
1 / 26
280 likes | 731 Views
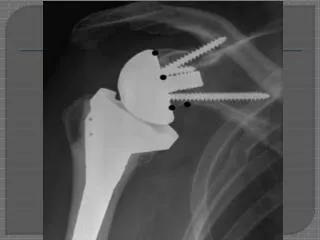
RESULTS AND COMPLICATIONS OF SHOULDER ARTHROPLASTY. James M. Steinberg, D.O. Types of Shoulder Arthroplasty. Hemiarthroplasty: humeral head replacement Constrained Total Shoulder Arthroplasty: ball-in-socket Unconstrained Total Shoulder Arthroplasty: anatomic or resurfacing

E N D
RESULTS AND COMPLICATIONS OF SHOULDER ARTHROPLASTY James M. Steinberg, D.O.
Types of Shoulder Arthroplasty • Hemiarthroplasty: humeral head replacement • Constrained Total Shoulder Arthroplasty: ball-in-socket • Unconstrained Total Shoulder Arthroplasty: anatomic or resurfacing • Tissue Ingrowth Total Shoulder Arthroplasty: bony and fibrous growth into the prosthetic elements
Indications for Shoulder Arthroplasty • Trauma: typically in three and four part proximal humerus fractures • Avascular Necrosis of the Humeral Head • Osteoarthritis • Rheumatoid Arthritis Goal: pain relief and restoration of movement
Hemiarthroplasty • Neer type of prosthesis has been available for over 40 years • Utilization in old trauma: - typically provides pain relief but incomplete motion - surgical procedure often difficult due to fibrosis of tissue and bone deformity
Hemiarthroplasty • Utilization in old trauma: • Tanner & Cofield(1983): 28 shoulders, 89% pain relief, avg. 112 degrees of active abduction, 1 nerve injury, 3 tuberosity/cuff problems, 2 instability, 1 ectopic bone • Hawkins et al.(1987): 9 shoulders, 67% pain relief, avg. 140 degrees of active abduction, no complications
Hemiarthroplasty • Utilization in AVN: - typically provides pain relief and near normal return of movement - rotator cuff and glenoid surface are usually intact Rutherford & Cofield(1987): 11 shoulders, 100% pain relief, 161 degrees of active abduction, no complications
Hemiarthroplasty • Utilization in osteoarthritis: • results similar to those found with AVN because the rotator cuff remains intact and a relatively painless articulation is created • Zuckerman & Cofield(1986): 36 shoulders, 83% pain relief, avg. 132 degrees of active abduction, no complications
Hemiarthroplasty • Utilization in rheumatoid arthritis: - pain relief often provided - return of motion depends on the extent of disease involvement of the rotator cuff and capsular tissues • Zuckerman & Cofield(1986): 36 shoulders, 89% pain relief, avg. 106 degrees of active abduction, 1 infection, 1 nerve injury, 1 fracture
Hemiarthroplasty • Complications are infrequent: - infection - nerve injury - iatrogenic fracture - ectopic bone formation - component failure and loosening
Hemiarthroplasty • Postoperative instability: - lack of healing of the capsule, rotator cuff, or tuberosities - excessively strong healing with abundant fibrosis • Careful reconstruction of the capsule and rotator cuff are crucial • Attention to physical therapy postoperatively • If above are followed, complications are uncommon
Constrained Total Shoulder Arthroplasty • Ball-in-socket prosthesis • Most studies have found that pain relief is satisfactory but return of motion, abduction is limited • Complication rate high • Semiconstrained/hooded glenoid components have been designed - results and complications similar to ball-in-socket device
Constrained Total Shoulder Arthroplasty Results • Coughlin et al.(1979): 16 shoulders, 100% pain relief, avg. 104 degrees of active abduction, 1 infection and 1 instability • Lettin et al.(1982): 40 shoulders, 90% pain relief, avg. 70 degrees of active abduction, 3 instability and 10 glenoid loosening • Gristina & Webb(1982): 20 shoulders, 100% pain relief, avg. 58 degrees of active abduction, 2 instability
Constrained Total Shoulder Arthroplasty Results • Brostrom et al.(1992): 23 shoulders, 65% pain relief, avg. 35 degrees of active abduction, 1 infection, 1 fracture, 1 instability, 3 glenoid loosening • Laurence(1991): 71 shoulders, 80% pain relief, avg. 76 degrees of active abduction, 1 instability, 1 glenoid loosening, 4 humeral loosening
Semiconstrained Total Shoulder Arthroplasty Results • Mazas & de la Caffiniere(1982): 32 shoulders, 91% pain relief, 3 infections, 1 nerve injury, 9 instability, 2 glenoid loosening • Amstutz et al.(1988): 10 shoulders, 100% pain relief, avg. 85 degrees of active abduction, 1 fracture, 1 glenoid loosening
Constrained Total Shoulder Arthroplasty • Complications: - infection - fracture - nerve injury - ectopic bone formation - dislocations - component loosening or material failure
Constrained Total Shoulder Arthroplasty • Majority of complications are instability and glenoid component loosening • Most dislocations and component failure require revision • Based on the high complication rate and lack of return of abduction, its use is rarely indicated
Unconstrained Total Shoulder Arthroplasty • Neer type of unconstrained TSA is the standard implant which others must be compared • Indicated in patients with OA, RA, and arthritis secondary to a previous trauma • No or slight pain is present in 90% of patients treated
Unconstrained Total Shoulder Arthroplasty • Patients with diagnosis of RA typically only have a return of active abduction about one half normal • Patients with diagnosis of OA typically only have a return of active abduction about three-fourths normal
Unconstrained Total Shoulder Arthroplasty Results • Neer et al.(1982): 194 shoulders, clinical ratings; 101 excellent, 28 satisfactory, 21 unsatisfactory, 43 limited rehabilitation, 1 infection, 1 fracture, 6 instability, 7 impingement/cuff/tuberosity problem • Cofield(1984): 73 shoulders, 92% pain relief, avg. 120 degrees of elevation, avg. 48 degrees of external rotation, 1 nerve injury, 6 impingement/cuff/tuberosity problem, 3 glenoid loosening • Barrett et al.(1989): 140 shoulders, 93% pain relief, avg. 90 degrees of elevation, avg. 40 degrees of external rotation, 2 nerve injury, 4 instability, 3 impingement/ cuff/tuberosity problem
Unconstrained Total Shoulder Arthroplasty Results • Hawkins et al.(1989): 70 shoulders, 90% pain relief, avg. 131 degrees of elevation, avg. 36 degrees of external rotation, 4 fracture, 1 instability, 2 impingement/cuff/tuberosity problem, 2 glenoid loosening • Boyd et al.(1991): 131 shoulders, 95% pain relief, avg. 100 degrees of elevation, avg. 33 degrees of external rotation, 2 fracture, 1 nerve injury, 2 instability, 1 glenoid loosening
Unconstrained Total Shoulder Arthroplasty Complications: -rotator cuff or tuberosity difficulties -instability -glenoid loosening -infection -intraoperative or postoperative fracture -nerve injury -ectopic bone formation
Unconstrained Total Shoulder Arthroplasty • Review of 1046 Neer total shoulder replacement the complication rate was 12%, majority being an impingement/ cuff/ tuberosity problem • Results are substantially better than the results of constrained or semiconstrained • Rate of revision is low, most commonly for glenoid loosening
Tissue Ingrowth Total Shoulder Arthroplasty • Developed by English & Macnab • Components are porous and allow for tissue ingrowth • Glenoid component has superior extension and therefore acts as a semiconstrained device • Pain relief was satisfactory in 85-90% of patients • Return of movement limited • Important to have adequate bone and joint stability
Tissue Ingrowth Total Shoulder Arthroplasty Results • Faludi & Weiland(1983): 13 shoulders, avg. 75 degrees of active abduction, 1 infection, 2 fractures, 1 instability • McElwin & English(1987): 13 shoulders, 85% pain relief, avg. 56 degrees of active abduction, 1 fracture, 1 instabilty, 3 component failures, 2 glenoid loosening • Mayo Clinic(83-86): 32 shoulders, 96% pain relief, avg. 145 degrees of active abduction, 1 infection, 2 glenoid loosening, 1 humeral loosening
Tissue Ingrowth Total Shoulder Arthroplasty Complications: slightly more common than in unconstrained implants -fracture -instability -component failure -component loosening
Summary • Hemiarthroplasty is effective in acute fractures, (3 and 4 part), and in AVN of the humeral head • If there is moderate glenoid involvement an unconstrained total shoulder arthroplasty is the better choice • Little indication for constrained or semiconstrained devices • With adequate bone, tissue ingrowth systems may be a viable alternative to cemented unconstrained systems