Download
1 / 24
390 likes | 1.22k Views
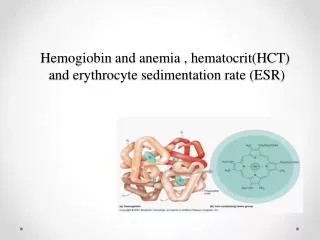
Erythrocyte Sedimentation Rate (ESR).

E N D
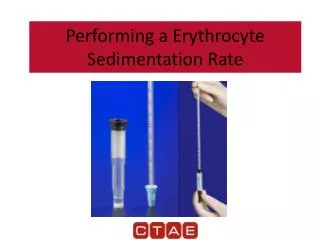
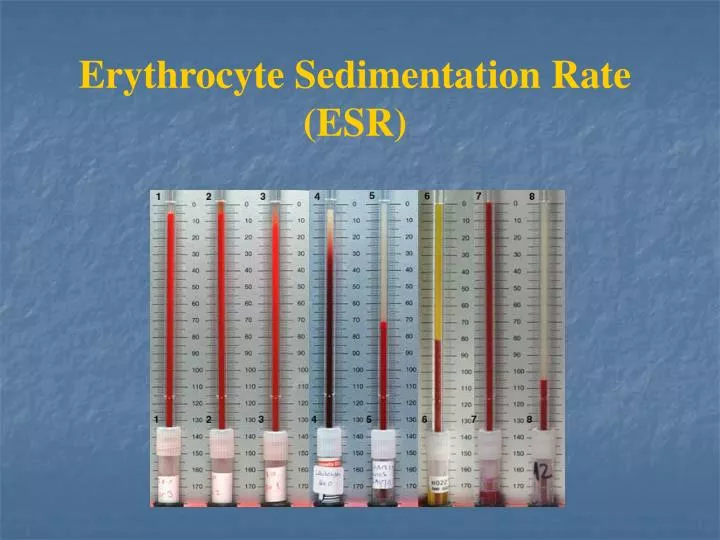
The erythrocyte sedimentation rate (ESR) is a nonspecific measurement used to detect and monitor an inflammatory response to tissue injury (an acute phase) in which there is a change in the plasma concentration of several proteins (termed acute phase proteins). This procedure, very simply, consist of allowing a specific amount of blood to sit in a vertical position for a period of time (usually one hour). The distance, in millimeters, that the red cells fall during this time period is the erythrocyte sedimentation rate and is reported in mm/hr. The ESR is affected by three factors: erythrocytes, plasma composition, and mechanical/technical factors.
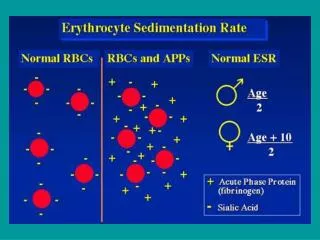
Erythrocytes • A factor of chief importance in determining the distance the RBCs fall is the size or mass of the falling particle. The larger the particle, the faster its rate of fall. • In normal blood, the RBCs remain more or less separated. They are negatively charged and, therefore repel each other. • In certain diseases, however, plasma protein concentration may be altered, causing a reduction in the negative charge of the RBCs and consequent formation of rouleaux. This leads to a larger mass and an increased sedimentation velocity. • Agglutination of RBCs due to change in the erythrocyte surface also leads to an increased RBC mass and a more rapid sedimentation rate.
Erythrocytes • Macrocytes tend to settle more rapidly than microcytes. RBCs show an alteration in shape, such as sickle cells and spherocytes, are unable to aggregate or form rouleaux and the sedimentation rate is decreased. • Anisocytosis and poikilocytosis reduce the ability of RBCs to form large aggregates and there by tend to falsely lower ESR. • In severe anemia, the ESR is markedly elevated: the concentration of RBCs is decreased, aggregation and rouleaux formation are increased, and they therefore, settle out more easily and rapidly. • In polycythemia, in which the RBCs count is high, the ESR is generally normal.
Plasma composition • The plasma composition is the most important factor determining the ESR. Rouleaux and aggregation of the RBCs are controlled primarily by the levels of acute phase proteins (most notable fibrinogen, -1 globulin, and -2 globulin); increasing these three plasma protein levels are increased in the plasma. • As the concentration of protein increases so does the viscosity of the plasma. Although an increased plasma viscosity will tend to inhibit the fall of the RBCs, the increase in plasma proteins are generally those which cause rouleaux and aggregation of the RBCs, which affects the ESR more greatly than does the increased plasma viscosity. Increased concentrations of albumin will tend to lower the ESR.
Mechanical/Technical factors • It is important that the ESR tube be exactly perpendicular. A tilt of 30 can cause errors up to 30%. • Also, the rack holding the tubes should not be subject to any movement or vibration. • Minor, everyday variations in room temperature do not significantly affect the ESR. With large changes in temperature, however, the sedimentation rate increases as the temperature increases. • The length and inner diameter of the ESR tube also affect the final test results. ESR tubes with a narrower than standard bore will generally yield lower sedimentation rates.
Normal values: Adult male 0-15 mm/hr Adult female 0-20 mm/hr
Significance of the ESR • The ESR represents a nonspecific response to tissue damage and inflammation and denotes the presence of disease, but not its severity. • It primarily reflects changes in the plasma proteins that accompany most the acute and chronic infections, tumors, and degenerative diseases. It may be used to follow the progress of certain diseases such as tuberculosis and rheumatoid arthritis.
An elevated ESR may be found in: Pregnancy (after the third month). Acute and chronic infections. Rheumatic fever. Rheumatoid arthritis. Myocardial infection. Nephrosis. Acute hepatitis. Menstruation. Tuberculosis. Hypothyroidism. Hyperthyroidism.
Adults over 60 years of age frequently have a slightly higher ESR value due primarily to decreased concentrations of plasma albumin. A decreased ESR will be present in: Polycythemia. Congestive heart failure. Hypofibrinogenemia. The presence of red blood cell abnormalities (poikilocytosis, spherocytes, and sickle cells).
Westergren method • Reagents and Equipment: • Westergren pipette calibrated in millimeters. The National Committee for clinical laboratory standards has set specific dimensions for the pipettes to be used: • Length = 300.5mm (+/-0.5mm) (in order to fit into standard racks) • External diameter = 5.5mm (+/-0.5mm) • Internal bore = 2.65mm (=/-0.15mm) • Graduated scale on pipette = 200mm (+/- 0.35mm) (Graduated lines of uniform thickness 0.2mm) • 3-westergern pipette rack. All racks should contain a leveling bulb in order to ensure that the position of tubes is vertical (+/-2o).
Reagents and Equipment • Westergren rack. • Disposable pipettes • Leveling plate for holding the Westergren rack • Timer.
Specimen • Whole blood (4 volumes) diluted with 0.109 M trisodium citrate (1 volume). Alternatively, 3ml whole blood anticoagulated with EDTA. (If this specimen type is used the whole blood [2.0ml] must be diluted with 0.85% w/v sodium chloride [0.5ml] prior testing).
Principle • Whole blood (4 volumes) anticoagulated with 0.109M trisodium citrate (1 volume), or EDTA anticoagulated blood (4 volumes) diluted with 0.85% sodium chloride (1 volume) is mixed, placed in a Westergren pipette, and allowed to stand for exactly 1 hour in a vertical position. The number of millimeters the red blood cells fall during this timed period constitutes the ESR. • The normal values for the modified Westergren ESR are 0 to 15 mm/hour for women, 0 to 10mm/hour for men, and 0 to 10mm/hour for children.
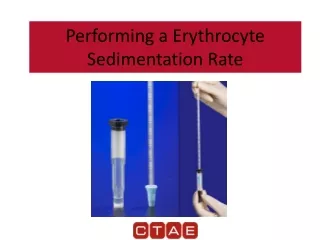
Procedures • 1-Mix the diluted blood for at least 2 minutes on a rotator. (The blood should be at room temperature). Check the tube for clots using two applicator sticks. • 2-Make certain the Westergren ESR rack is exactly level. • 3- Fill the Westergren pipette to exactly the 0 mark. Making certain there are no air bubbles in the blood. • 4-Place the pipette in the rack. Be certain the pipette fits snugly and evenly into the grooves provided. • 5-Allow the pipette to stand for exactly 60 minutes. • 6-At the end of 60 minutes records the number of millimeters the red blood cells have fallen. This result is the erythrocyte sedimentation rate in millimeters/hour
Wintrobe and Landsberg method • Reagent and equipment: • Wintrobe tube, calibrated in millimeters • Wintrobe pipette rack. • Disposable capillary pipette. • Applicator sticks • Specimen: • Whole blood, 1 ml, using EDTA as the anticoagulant.
Principle: Well-mixed, whole blood is placed in a Wintrobe tube and allowed to stand for 1 hour. The number of millimeters the red blood cells fall during time constitutes the ESR. In the Wintrobe and Landsberg method, normal values for women are0 to 20 mm/hour and 0 to 9 mm/hour for men.
Procedure: Mix the whole blood for at least 2 minutes on a rotator. (Make certain the blood is at room temperature). Check the tube for clots using tow applicator sticks. With a capillary pipette, fill the Wintrobe tube to the 0 mark. Place the tube in an exactly vertical position in the rack. Time for 60 minutes. At the end of 60 minutes, record the level of the erythrocyte column. This result is the erythrocyte sedimentation rate in millimeters/hour.
Discussion • The sedimentation of red blood cells takes place in three stages: • In the first 10 minutes (lag phase) rouleaux formation occurs and the sedimentation rate is slight. • Sedimentation then occurs for a period of approximately 40 minutes at a more rapid and constant rate (decanation). • During the last 10minutes, the sedimentation rate is slow because of the accumulation of RBCs in bottom of the tube. The longer the tube the longer the stage two will last, and therefore the higher the ESR result.
Discussion • Although care may be taken in filling the sedimentation tube to the 0 mark, occasionally the upper level of the blood may only reach the 1 or 2 mm mark. In such case, care should be taken when making the final reading. Subtract the 1 or 2 mm from the final result. For example, if the ESR tube is filled to the 2 mm mark and the RBCs fall to the 18mm mark, the ESR is reported as 16mm/hour. If the level of blood falls below the 5 mm mark, the test should be repeated to ensure that valid results are obtained. If the upper level of the blood is below 0 due to leakage of the blood from the bottom of the tube (Westergren method) the test must be repeated from step 1. leakage of blood from the bottom of the tube invalidates the test result.
Discussion • All the sedimentation racks should be equipped with leveling screws and a spirit level. • Mechanical sources of error: • If the concentration of EDTA is greater than recommended, the ESR will be falsely low. • The anticoagulants sodium or potassium oxalate and heparin cause the RBCs to shrink and the ESR will be falsely high. • If the ESR stands for more than 60 minutes, the results will be falsely elevated. If the test is timed for less than 60 minutes, invalidly low values are obtained. • A marked increase (or decrease) in room temperature leads to increased (or decreased) ESR result. • Tilting of the ESR tube increases the ESR. • Bubbles in blood cause invalid results. • Fibrin clots present in the blood invalidate the test results.
Discussion • The ESR should be set up within 2 hours of blood collection. If EDTA is used as the anticoagulant, the test may be set up within 6 hours if the blood has been refrigerated. • The Wintrobe ESR technique is thought to be more sensitive when the ESR is low, whereas the Westergren procedure more accurately reflects the patient’s disorder when the results are high. The Westergern method has been chosen as the standard method by the International Committee for Standardization in Hematology.
Discussion • When reading the ESR results on bloods with an extremely high WBCs or platelet count, the buffy coat should be excluded from the reading. • If there is poor separation of the RBCs and plasma layers this may be due to an increased number of reticulocytes and has been termed “stratified sedimentation”. • The internal bore and the length of the graduated scale on the Westergern pipette are critical measurements.
Disposable ESR • commercial kits are now available for a disposable ESR test. Several kits include safety caps for the pipettes that allow the blood to precisely fill to the zero mark. This makes the pipette a closed system and eliminates the error involved with manually setting the blood at the zero mark.