Download
1 / 19
190 likes | 210 Views
Detailed examination of RBMC's policy on restraint use, forthcoming changes, types of restraints, devices, application methods, and patient rights. Guidelines for restraint orders and classifications provided.

E N D
Objectives Restraints Update 2014 Review types of restraints Review RBMC policy and forthcoming changes regarding use of restraints & seclusion Review documentation and forms: Physician Order form, Restraint flow sheet, Occurrence Screening form Review correct application of restraint devices: Chest posey/vest and limb restraints
RBMC Philosophy • Patients have the right to be free of restraints • Limited only to clinically justified situations. • Will be discontinued at the earliest possible time based on the re-evaluation of the patient’s condition. • Not determined by the treatment setting or the patient’s diagnosis but by the situation the restraint/seclusion is intended to address.
What are Restraints? • Any manual methods, physical or mechanical device, material or equipment that immobilizes or reduces the ability of a patient to move his or her arms, legs, body, or head freely; or • A drug or medication used as a restraint to manage the patient’s behavior or restrict the patient’s freedom of movement and is not a standard of treatment or dosage for the patient condition
Restraint Devices • Body Restraints Vest (Chest Posey) • Soft Limb Restraints Hand Mitts Wrist Ankle • Freedom Splint • Leather Restraints 4 point 3 point 2 point • Medications • Seclusion • 4 Side rails up • Only approved manufactured products are to be used as restraints • If possible, try alternatives to restraints before using restraints Least restrictive Most restrictive • Leather restraints can be applied for safety if the patient’s size or presentation would render a cloth restraint ineffective.
*Physical Hold for Forced Medications • The application of force to physically hold a patient in order to administer a medication against the patient’s wishes. • Must have a physician’s order prior to application of the restraint (use of force). • If physical holding for forced medications is necessary with a violent patient, the one hour face to face evaluation is required. *Forthcoming changes in the policy
The following are NOT considered restraints • Temporary immobilization for medical, dental, diagnostic, or surgical procedures • Methods to hold a patient during routine exam/procedures as long as pt’s right to refuse the procedure is honored • IV board used to maintain IV access • Adaptive support devices such as postural supports or orthopedic appliances • Side rails on a stretcher • Developmentally appropriate safety devices such as stroller safety belts, high chair lap belts, raised crib rails or crib covers • Hand mitts unless pinned or attached to the bed, or if applied so tightly that hands & fingers are immobilized. • Medications that are used as part of a patient’s standard medical or psychiatric treatment and are administered within the standard dosage for the patient’s condition.
*Side Rails up • If a patient is not physically able to get out of bed regardless of whether the side rails are raised or not, raising all 4 side rails for this patient would not be considered restraint because the side rails have no impact on the patient’s freedom of movement. • In this example, the use of all 4 side rails would not be considered a restraint. • 4 side rails up are not considered restraints when patient is sedated or experiencing involuntary movements, or is on seizure precautions. *Forthcoming changes in the policy
Restraint Orders • Reason for restraint • Type of restrain • Order parameters • Physician Assessment (One hour face to face assessment) • Must be signed by a licensed independent practitioner • NEVER written as a standing order or prnorder • If a patient was recently released from restraints and exhibits behavior that can only be handled by reapplication of restraints, a new order is required. • NOTE: Another face-to-face evaluation by the LIP is required if the restraint is to continue past 24 hours.
Classification of Restraints Non-Violent or Non Self-Destructive Violent or Self-Destructive Behavior • Order parameter: Daily • Face to face evaluation by LIP *(1 hour time frame does not apply) • Visual observation and documentation at least q 2 hrs • If on chest posey/vest, visual observation during sleep time 10pm-6am is at least q 1 hr • Order parameters: Adults: 4 hours Children 9-17 yrs old: 2 hours Children < 9 yrs old: 1 hour • Face to face evaluation by LIP w/in 1 hour of initiation of restraint • Continuous monitoring • Documentation at least q 15 min LIP: Licensed Independent Practitioner *Forthcoming changes in the policy
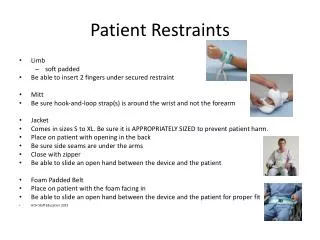
How to apply Restraints Should be… • Applied in a way that allows for quick release/removal • Snug but not too tight – should be able to insert 1 to 2 fingers between the wrist/ankle restraint and the patient’s limb. • Secured to the movable part of the bed, stretcher frame, or chair frame according to the manufacturer’s guidelines • Should never be secured to the side rails • If feasible, the bed should be kept in low position with the wheels locked.
Seclusion • Involuntary confinement of a patient alone in a room or area from which the patient is physically prevented from leaving • Seclusion may only be used for the management of violent or self-destructive behavior that jeopardizes the immediate physical safety of the patient, staff member or others Seclusion rooms are located in the CLI and CSU *In all other areas, if a pt. is restricted to a room alone and staff is physically intervening to prevent the patient from leaving the room or giving the perception that threatens the pt. with physical intervention if the patient attempts to leave the room, the pt. is being secluded. *Forthcoming changes in the policy
Debriefing • Debriefing of patients released from restraints for violent or self-destructive behavior will occur as soon as appropriate but not more than 24 hours after the restraint/seclusion episode. • Discussion includes: • Factors that led to the restraint/seclusion • Steps to reduce the potential for future need of restraint/seclusion • Clinical impact on the patient • Identification of ways the situation could have been handled differently • Document the debriefing meeting on the Restraint Flow Sheet.
Occurrence Screening Form • Complete this form for patients in restraints for violent or self-destructive behavior for more than 12 hours or if pt. has 2 or more episodes of restraint use for violent or self destructive behavior within 12 hours. • Send to the Clinical Outcomes Dept. • A copy is sent to the Director of Nursing Quality, Research, and Resources.
Assessment & Monitoring – Responsibility of the RN • Revaluation of the need for restraints at least every 2 hrs. • Toileting at least every 2 hrs • Release of restraints at least every 2 hrs: circulation checks, skin assessment and care, ROM for a minimum of 5 minutes per limb. • Meals and fluids at least 3x a day, more often if necessary • Assistance with bathing at least once per day • Ambulation at least once every 4 hrs, if clinically feasible Documentation – Restraint Flow Sheet • Should match the rationale for continued use, e.g. patients noted to be awake, oriented and cooperative should not still be restrained. • Modify Interdisciplinary Plan of Care to reflect use of restraints/seclusion • Update Kardex
Informing Patient and Family • Inform patient of the plan of care and rationale for using restraints/seclusion, if clinically feasible. • Document on the Restraint Flow Sheet. • Notify patient’s family/guardian/healthcare decision maker • This notification will be done as soon as possible after the initiation of restraints/seclusion, but no longer than 24 hours after application. • Document on the Restraint Flow Sheet and in the Nurses’ Notes.
Forensic Restraint • Handcuffs, manacles, shackles, and other chain type restraint devices used for custody, detention, and public safety reasons. • Used only for patients in the custody of the police and the Department of Corrections and is not governed by the restraints policy. • RBMC is still responsible for appropriate patient assessment and provision of safe appropriate care (with law enforcement officer prisoner).
Reportable Events Serious, preventable adverse events, as well as death, are reportable events. • Any patient death, loss of body part, disability, or loss of bodily function lasting more than 7 days or still present at discharge is considered a Serious Preventable/potentially Preventable Adverse Event. This includes incidents associated with the use of restraints. Any death that occurs under the following circumstances must be reported to the Center for Medicare and Medicaid Services (CMS) • Every death that occurs while the patient is in restraints/seclusion. • Every death that occurs within 24 hours after the patient has been removed from restraints/seclusion. • Every death known to the hospital that occurs within 7 days after restraints/seclusion where it is reasonable to assume that the use of restraint or placement in seclusion contributed directly or indirectly to a patient’s death.