Download
1 / 61
610 likes | 623 Views
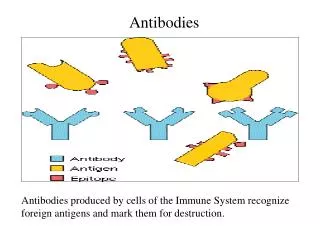
Explore the evolution of monoclonal antibodies in medical treatment, from historical uses to modern applications in allergic diseases and cancer therapy. Learn about hybridoma selection, species-specific antibodies, and the potential for treating human diseases using MAbs. Gain insights into immunotherapy concepts and their impact on human health.

E N D
Antibodies as Therapeutic Entities Duncan Hannant Animal Health Trust Newmarket
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
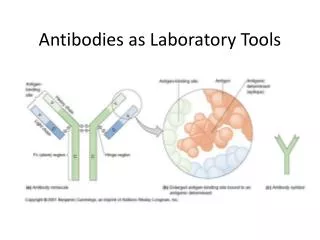
Monoclonal antibodies: Summary Hybridoma selection based on drug resistance • Identify immortalised mouse myeloma cell line (e.g. NS1 myeloma derived from BALB/c mice) • Mutate to make deficient in enzymes necessary for DNA synthesis (HGPRT and TK) HGPRT = hypoxanthine-guanine phosphoribosyltransferase TK = thymidine kinase
Monoclonal antibodies: Summary Hybridoma selection based on drug resistance • Mutated myeloma cells will not grow in presence of aminopterin. • Fuse myeloma cells to normal B cells from immunised mouse (PEG used routinely now) • Unfused myeloma cells die (aminopterin) • Unfused normal B cells die after 1-2 weeks anyway • Only hybridomas survive (they can use hypoxanthine and thymidine).
Biosynthetic mutations in mutant myeloma cells EnzymePresentAbsentResult HGPRT ×Can’t use hypoxanthine TK ×Can’t use thymidine Rescue path Can use Uridine BUT: Culture medium contains HAT which blocks the Rescue Pathway H = hypoxanthine A = aminopterin T = thymidine
Species-specific monoclonal antibodies: summary • Very few human myeloma cell lines • Even less myeloma cell lines in other species • Inter-species fusions are possible but give low hybridisation frequency and unstable hybrids Possible Solution: Use heterohybridoma cell lines as fusion partners
Species-specific Mabs: basic method e.g. Consider the horse Antibodies produced from: (Horse x Mouse) x Horse Heterohybridomas Examples of equine antibodies to influenza virus (previous lecture)
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
Historical: Antibodies used in passive therapy • Anti-tetanus antibodies derived from horses (>100 years ago). • Anti-toxin (e.g. snake venom etc). • Intravenous injection of maternally derived antibodies into neonates (failure of colostral transfer - many animals). • Infusion of immune serum into diseased animals (e.g. Rhodococcus equi in foals). • Immunised goat serum components (HIV and MS)
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
Immunotherapy • Based on the body’s natural defense system. • Enhance this response ~ cancer therapy. • Reduce this response ~ asthma therapy. • Cytokine and MAb therapy are commonplace in cancer treatment. • Cytokine enhancement of anti-virus responses/vaccines are common in vet science.
Non-specific immunotherapy • Stimulators of immune responses (biological response modifiers). • Coley’s vaccine (~1900, gruesome, Streps and Staphs) • BCG (1922 - equally so, granulomas etc) • Strange things: goat serum, heterologous proteins, quartz and other particulates.
Pathogen related/specific immunotherapy (i) • Interferon alpha (IFN-alpha, effective in virus diseases and cancers such as multiple myeloma, chronic myeloid leukemia, malignant melanoma). • Cytokines e.g. IL-2 (kidney cancer and melanoma) IL-2, IL-6 (adjuvants in virus vaccines, enhancing anti-tetanus responses in aged people) and TNF-alpha. • Side effects can be significant. • Cancer vaccines: cancer antigen(s) + other components - e.g. anti-idiotypic MAbs for colorectal cancer (QMC Nottingham - see later) Ref: Durrant LG and Spendlove I (2003) Cancer vaccines entering Phase III clinical trials. Expert Opin. Emerg. Drugs 8, 489-500.
Pathogen related/specific immunotherapy (ii) Monoclonal antibodies • Becoming useful in allergic disease treatment • Now part of standard cancer treatment • Potential as “guided missile” delivery systems for drugs, toxins etc.
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
Factors affecting the use of MAbs in therapy: General • Extremely high target specificity but antibodies are large proteins c.f. drugs. • Slow kinetics of distribution. • Limited tissue-penetration. • Dependent upon blood supply to locate to solid tumours. • Dependent upon high level of target antigen expression (and its accessibility) in tumours. • Dependent upon MAb isotype, avidity etc.
Factors affecting the use of MAbs in therapy: Mab efficacy • Often not completely known, many bystander effects. • Blocking function of target antigen. • Killing target cell (cytotoxicity) • Complement activation (cytotoxicity) • Recruitment of phagocytes/NK cells etc. • Blocking/activating a receptor for intracellular signal transduction (e.g. NF-kappaB) • Transport of toxins, drugs, radionuclides to diseased tissues. • Recombinant peptide inclusion in MAb (e.g. TNFalpha antagonist, Etanercept).
Factors affecting the use of MAbs in therapy: Problems (i) • Mouse Fc may not interact with human FcR: reduced effector function. • Rapid clearance of foreign protein from bloodstream. • Development of human anti-mouse antibodies (HAMA). • Retreatment could result in anaphylaxis/allergy • Retreatment could be less effective than previous treatments. • NB: What about positive benefits of HAMA? • De Nardo GL et al (2003) Human antiglobulin response to foreign antibodies: therapeutic benefit? Cancer Immunol. Immunother. 52, 309-316 (Printed copy of abstract supplied)
Factors affecting the use of MAbs in therapy: Problems (ii) • First injection induces multiple systemic symptoms (chills, headache, pyrexia, vomiting, diarrhoea, tachycardia, respiratory distress, hypotension, arthralgia) - common with OKT3 (anti CD3) and Campath-1-H (anti CD52), also seen with TNFalpha antagonists. • Due to massive systemic cytokine release after T cell activation by MAbs. • OKT3 also induces C’ activation. • NB:these are reversible and not life-threatening.
MAbs in therapy: Overcoming some problems Q: How can we reduce the problem of HAMA? A1: Chimeric MAbs (ag binding = mouse, effector function = human) A2: Humanised MAbs (replace resident hypervariable region with new amino acids) A3: Transgenic mice (human Ab gene loci inserted into body by embryonic stem cell transfer) A4: “Knock-out” mice with Ab producing genes deleted.
MAbs in therapy: Overcoming some problems Potential of transgenic mouse approaches to reduce HAMA are: • Mouse can be immunised with desired antigen. • Mouse produces human antibodies. • ASC can be fused with myeloma cells to produce all-human MAbs.
Some current applications of MAbs in disease therapy • Inhibition of alloimmune reactivity (graft rejection). • Inhibition of autoimmune reactivity (RA, Crohn’s disease, SLE). • Allergic lung disease therapy. • Cancer therapy. • Infectious disease therapy (RSV). • Antiplatelet therapy (acute coronary syndromes) • NB: 25% of all biotech drugs in R&D are MAbs - >30 in clinical evaluation now.
Some current applications of MAbs in disease therapy • Inhibition of alloimmune reactivity (graft rejection). • Ortho Multicentre Transplant Study Group: A randomised clinical trial of OKT3 monoclonal antibody for acute rejection of cadaveric renal transplants. N. Eng. J. Med. 1985, 313, 337-342. • Kahan BD et al. Reduction in occurrence of acute cellular rejection among renal allograft recipients treated with basilimixab, a chimeric anti-interleukin-2 receptor monoclonal antibody. Transplantation 1999, 67, 276-284. • Vincenti F et al. Phase I trial of humanised anti-interleukin-2 receptor antibody in renal transplantation. Transplantation 1997, 63, 33-38.
Some current applications of MAbs in disease therapy • Inhibition of autoimmune reactivity (RA, Crohn’s disease, SLE). • Maini RN et al. Infliximab (chimeric anti-TNFalpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. Lancet 1999, 354, 1932-1939. • Breedveld FC. New TNFalpha biologic therapies for rheumatoid arthritis. Eur. Cytokine Netw. 1998, 9, 233-238. (Etanercept, IgG1 fusion protein) • Geletka RC, St Clair (2005) Infliximab for treatment of early rheumatoid arthritis Expert Opin. Biol. Ther. 5, 405-407. (MAb against TNF)
Some current applications of MAbs in disease therapy • Infectious disease therapy (RSV). • Malley R et al. Reduction of respiratory syncytial virus (RSV) in tracheal aspirates in intubated infants by use of humanised monoclonal antibody to RSV F protein. J. Inf. Dis. 1998, 178, 1555-1561 (Palivizumab - Synagis) • Mejias A et al (2004) Asthma and RSV: new opportunities for therapeutic intervention. An. Pediatr. (Barc) 61, 252-60 (use of MAB against RSV in patients).
Some current applications of MAbs in disease therapy • Antiplatelet therapy (acute coronary syndromes). • Hamm CW et al. Benefit of abciximab in patients with refractory unstable anginain relation to serum troponin T levels. c7E3 Fab Antiplatelet Therapy in Unstable Refractory Angina (CAPTURE) Study Investigators. N. Eng.J Med. 1999, 340, 1623-1629 (based on MAb to platelet receptor, gpIIb/IIIa). • Note: Two clinical trials with placebo stopped because of highly significant benefit.
MAbs in disease therapy • In all these cases, a reduction in immunogenicity is seen with MAbs in this order: Murine Chimera Humanised Human
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources
Humanised Mab Therapy: Asthma • Monoclonal antibodies made against human IgE. • Antibodies selected that bound to FcεR1-binding region of free IgE. • The MAbs formed complexes with free IgE: stopped attachment to mast cells and basophils. • Problems with allergic responses and reduced therapeutic efficacy (cleared quickly) because MAbs were immunogenic.
Humanised Mab Therapy: Asthma • MAbs to IgE molecule. • MAbs to IL-5
Humanised Mab Therapy: Asthma • Recombinant humanised MAb to IgE (Omalizumab) prepared which also cleared free IgE from circulation. • Resulted in a dose-related and sustained fall in plasma IgE. • Reduced early bronchoconstriction responses to inhaled allergen were seen but also the late responses (T cell and eosinophil mediated). • Also, showed reduction in high affinity IgE receptors on circulating basophils (because levels of IgE in circulation regulate FcεR1 in vivo)
Humanised Mab Therapy: Asthma • Very low occurrence of adverse side reactions to Omalizumab (humanised). • Immune complexes of MAb/IgE cleared by reticuloendothelial system (no kidney damage). • Although rather expensive, only 5% allergic patients have severe asthma. Cost is acceptable c.f. alternatives (steroids, oral gold, other drugs - high frequency of toxicity) • See Holgate et al (2005)paper: next slide
Humanised Mab Therapy: Asthma Mab to IL-5 • IL-5 ~ eosinophilic inflammation of asthma. • IL-5 gene deletion or anti-IL-5 MAbs markedly reduce eosinophilic inflammation and airway reactivity in mice. • Anti-IL-5 MAb effects last for 3 months in primates (chronic asthma therapy possible?). • Humanised anti-IL-5 MAb (Mepolizumab) reduces blood eosinophils by >95% but only 50% in lung. No significant clinical benefit. • Needs more work!
Gibson SG Standard 1973
Summary of this Session • Part 1: Rapid review of mouse and species-specific MAbs. • Part 2: Historical - antibodies in therapy e.g. “antiserum”, antitoxins, passive transfer. • Part 3: Concepts of Immunotherapy - biological response modifiers, immune enhancers, immune suppressors, MAbs. • Part 4: MAbs used in human medicine - general approaches, problems, applications and benefits. • Part 5: MAbs in Allergic Human Disease. • Part 6: MAbs in Cancer Therapy. • Part 7: Student discussion on potential of MAbs for treatment of human diseases. • Part 8: Resources 0.75
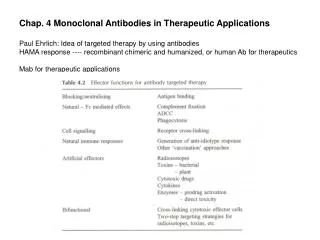
MAbs in Cancer Therapy Subject areas previously covered in lectures: • Design of MAbs • MAb-cytotoxic agent conjugates • Pharmakokinetics • Immunogenicity. • Engineering antibody molecules for therapy (Dr Clarke) • Applications of engineered antibodies (Dr Clarke) • Engineering antibodies for human therapy (Dr Athwal)
MAbs in Cancer Therapy Two examples described: • Lymphoma therapy (Lym-1 and Lym-2) • Cancer vaccine (anti-idiotype for colorectal cancer - Licenced from CRC as Onyvax-105)
MAbs in Cancer Therapy Lymphoma therapy with MAbs Lym-1 and Lym-2. • Tumour cell nuclei used as immunogens. • Mouse MAbs reactive with B cells (tumour and normal) but not myeloid cells, or T cells. • Target antigen is HLA-DR (discontinuous epitope on beta chain of HLA-DR10, but also other DRs) • Selectivity for lymphoma cells on basis of target antigen density and MAb avidity. • Further details: see notes in “Resources” section.
MAbs in Cancer Therapy Cancer vaccine (anti-idiotype for colorectal cancer) Smart news from Nottingham! • Human monoclonal anti-idiotypic antibody made which mimics a TAA (CD55) on colorectal cancer. • Phase I trial: non-toxic, enhanced patient survival. • Stimulates anti-tumour T cell responses (Th1 and increased IL-2 production). • T and NK cell invasion of solid tumours seen (very valuable). • Sequencing of the anti-idiotype and CD55 shows that patients with HLA-DR1, DR3 and DR7 should show enhanced T cell responses to tumour.
MAbs in Cancer Therapy Cancer vaccine (anti-idiotype for colorectal cancer) Continued: • 83% patients carrying these HLA-DR haplotypes responded to this vaccine. • 88% patients not expressing these haplotypes were non-responders. • Onyvax started Phase II trials in 2000 • Ref: Durrant LG et al (2000) A neoadjuvant clinical trial in colorectal cancer patients of the human anti-idiotypic antibody 105AD7, which mimics CD55. Clin. Cancer Res. 6, 422-430. • See also Pritchard-Jones et al (2005) use of 105AD7 in osteosarcoma (next slide)