Download
1 / 56
590 likes | 700 Views
Discover the crucial role electrolytes play in various bodily functions, including maintaining water balance, regulating pH levels, and supporting muscle and nerve function. Learn about key electrolytes, their functions, and clinical significance. Explore the body's complex systems for monitoring and balancing electrolyte concentrations.

E N D
Electrolytes Part 1
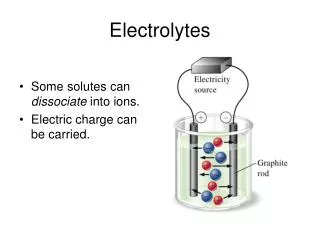
Cathode Anode Electrolytes • Electrolytes are ions capable of carrying an electricl charge • Anions: (-) → Anode • Cations: (+) → Cathode • Major cations of the body • Na+, K+, Ca2+ & Mg2+ • Major anions of the body • Cl-, HCO3-, HPO42- & SO42- M. Zaharna Clin. Chem. 2009
Essential Component in Numerous processes • Volume and osmotic pressure (Na+, K+, Cl-) • Myocardial rhythm and contraction (K+, Mg2+, Ca2+) • Cofactors in enzyme activation (Mg2+, Ca2+, Zn2+). • Regulation of ATPase ion pump (Mg2+) • Acid/Base balance (pH) (HCO3-, K+, Cl-) • Coagulation (Mg2+, Ca2+) • Neuromuscular (K+, Mg2+, Ca2+) The body has complex systems for monitoring and maintaining electrolyte concentrations M. Zaharna Clin. Chem. 2009
Maintenance of water homeostasis is vital to life for all organisms • Maintenance of water distribution in various body fluids is a function of electrolytes (Na+, K+, Cl- & HCO3-) M. Zaharna Clin. Chem. 2009
Water • Average water content of human body is 40-75% of total body weight. • Solvent for all body processes • Transport nutrients to cells • Regulates cell volume • Removes waste products → urine • Body Coolant → sweating • Water is located in intracellular and extracellular compartments • Intracellular fluid (ICF) is the fluid inside the cells • Extracellular fluid (ECF) and subdivided into the • intravascular extracellular fluid (plasma) • and the interstitial cell fluid that surrounds the cells in the tissue M. Zaharna Clin. Chem. 2009
Water • Normal plasma ~ 93 % H2O, the rest is mixture of Lipids and proteins. • Concentration of ions within the cells and plasma is maintained by: • Energy consumption: Active transport • Diffusion: Passive transport • Maintaining conc. of electrolytes affect distribution of water in compartments • Most membranes freely permeable to water • Conc. of ions on one side affect flow of water across the membrane M. Zaharna Clin. Chem. 2009
Osmolality • Physical property of a solution is based on the concentration of solutes per kilograms of solvent. (mOsm/Kg) • Sensation of thirst & arginine vasopressin hormone (AVP) [formerly, Antidiuretic hormone (ADH)] are stimulated by hypothalamus in response to increased blood osmolality • Thirst → more water intake • AVP → increase water absorption in kidney M. Zaharna Clin. Chem. 2009
Clinical Significance • Osmolality is the parameter to which hypothalamus responds to maintain fluid intake. • The regulation of osmolality also affects the Na+ concentration in plasma • account for ~90% of osmotic activity in plasma • Another process which affects Na+ concentration is regulation of blood volume. M. Zaharna Clin. Chem. 2009
Clinical significance • To maintain normal plasma osmolality (275-295 mOsm/Kg) hypothalamus must respond quickly to small changes • 1-2% increase in osmolality: 4 fold increase in AVP secretion. • 1-2% decrease in osmolality: shuts off AVP secretion. • Renal water regulation by AVP and thirst play important roles in regulating plasma osmolality. • Renal water excretion is more important in controlling water excess, • whereas thirst is more important in preventing water deficit or dehydration. • Consider what happens in several conditions. M. Zaharna Clin. Chem. 2009
Water Load • Excess intake of water lower plasma osmolality • Kidney is important in controlling water excess • AVP and thirst are suppressed • Water is not reabsorbed, causing a large volume of dilute urine to be excreted • Hypoosmolality and hyponatremia usually occur in patients with impaired renal excretion of water M. Zaharna Clin. Chem. 2009
Water deficit • As a deficit of water, plasma osmolality begins to increase • Both AVP secretion and thirst are activated. • Although AVP contributes by minimizing renal water loss, thirst is the major defense against hyperosmolality and hypernatremia. • A concern in infants, unconscious patients, or anyone who is unable to either drink or ask for water M. Zaharna Clin. Chem. 2009
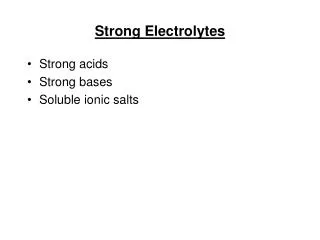
Regulation of blood volume • Blood volume essential in maintaining blood pressure and ensure perfusion to all tissue and organs. • Regulation of both sodium & water are interrelated in controlling blood volume • Renin-angiotensin-aldosterone: system of hormones that respond to decrease in blood volume and help maintain the correct blood volume. M. Zaharna Clin. Chem. 2009
Regulation of blood volume • Changes in blood volume is detected by receptors in: • the cardiopulmonary circulation , • carotid sinus, • aortic arch • and glomerular arterioles • They activate effectors that restore volume by: • appropriately varying vascular resistance, • cardiac output, • and renal Na and H2O retention. M. Zaharna Clin. Chem. 2009
Angiotensin converting enzyme (ACE) M. Zaharna Clin. Chem. 2009
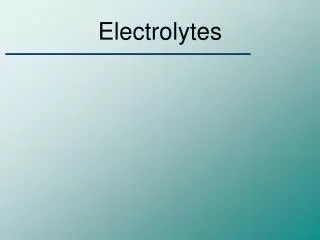
Regulation of blood volume • Other Factors effecting blood volume: • Atrial natriuretic Peptide (ANP) → sodium excretion → blood volume • Volume receptors → release of AVP → conserve water → blood volume • Glomerular filtration rate (GFR) in volume expansion and in volume depletion M. Zaharna Clin. Chem. 2009
Increase in Blood Volume M. Zaharna Clin. Chem. 2009
Determination of Osmolality • Serum or urine sample (plasma not recommended due to the use of anticoagulants) • Based on properties of a solution related to the number of molecules of solutes per kilogram of solvent such as: • Freezing point ( osmolality freezing point temp.) • Vapor pressure ( osmolality Vapor pressure) M. Zaharna Clin. Chem. 2009
Determination of Osmolality • Freezing Point Osmometer: • Standardized method using NaCl reference solution. • Specimen is supercooled to -7ºC, to determine freezing point • osmolality causes depression in the freezing point temp. • More solutes present the longer the specimen will take to freeze. M. Zaharna Clin. Chem. 2009
OsmolalGap • Osmolal gap is the difference between the measured osmolality and the calculated one. Osmolal Gap= measured osmolality - calculated osmolality • The osmolal gap indirectly indicates the presence of osmotically active substances other than sodium, urea or glucose. (ethanol, methanol or β-hydroxybutyrate) M. Zaharna Clin. Chem. 2009
Case Study • A sixty-seven year old white male was found pulseless and resuscitated; then brought to the emergency room. He had been reported to be drinking in a bar all afternoon, and had then fallen from a ten foot balcony to snow covered ground. He arrived in the emergency room with a fractured occiput and was unresponsive. • Admission Lab. results: M. Zaharna Clin. Chem. 2009
Case Study Cal. Osmo. = (2 X 143) + (104/20) + (4/3) = 286 + 5.2 + 1.33 = 293 Osmolal Gap= measured osmolality - calculated osmolality = 356 – 293 = 63 • An OG value greater than 15 is considered a critical value • The presence of low blood pH, elevated anion gap and greatly elevated OG is a medical emergency that requires prompt treatment M. Zaharna Clin. Chem. 2009
Sodium • Most abundant extracellular cation- 90% • Major function is maintaining the normal water distribution & osmotic pressure of plasma • Role in maintaining acid-base balance (Na+, H+ exchange mechanism) • Normal range Serum: 136-145 mmol/L • ATPase ion pump: the way the body moves sodium and potassium in and out of cells. • 3 Na+ out of the cell for every 2 K + in and convert ATP to ADP. M. Zaharna Clin. Chem. 2009
Regulation of Sodium Balance • Plasma Na+ concentration depends: • on the intake and excretion of water • and, on the renal regulation of Na+ • Three processes are of primary importance: • Intake of water in response to thirst ( p. osmolality) • The excretion of water (AVP release) • The blood volume status, which affects Na+ excretion through aldosterone, angiotensin II, and ANP (atrial natriuretic peptide). M. Zaharna Clin. Chem. 2009
Regulation of Sodium Balance • 70 % of sodium that is filtered is reabsorbed in proximal tubules. • Remainder occurs in the ascending loop of Henle (without water absorption) & DCT under regulation of: • Aldosterone • Renin-Angiotensin system • Atrial natriuretic Peptide (ANP) → sodium excretion M. Zaharna Clin. Chem. 2009
Hyponatremia • Defined as a serum/plasma level less than 135 mmol/L. • One of the most common electrolyte disorders in hospitalized and non-hospitalized patients • Levels below 130 mmol/L are clinically significant. M. Zaharna Clin. Chem. 2009
Hyponatremia M. Zaharna Clin. Chem. 2009
Hypernatremia • Hypernatremia: increased sodium concentration > 145 mmol/l • Result of excess water loss in the presence of sodium excess, or from sodium gain M. Zaharna Clin. Chem. 2009
Sodium determination • Methods: • Flame emission spectrophotometry • measurement of light emitted when the element is excited by energy in the form of heat. M. Zaharna Clin. Chem. 2009
Atomic absorption spectrophotometry M. Zaharna Clin. Chem. 2009
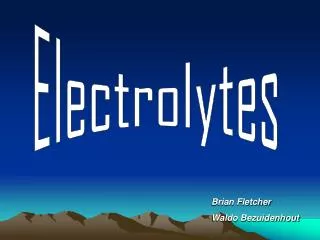
Ion Selective electrode Reference electrode selective membrane at the ion selective electrode, allows measured ions to pass, but excludes the passage of the other ions M. Zaharna Clin. Chem. 2009
Potassium • Major intracellular cation • 20 X greater concentration in the cell vs. outside. • 2% of the bodies potassium circulates within the plasma. • Function: • Regulates neuromuscular excitability • Hydrogen ion concentration • Intracellular fluid volume M. Zaharna Clin. Chem. 2009
Effects on Cardiac muscle • Ratio of K+ intracellular & extracellular is important determinant of resting membrane potential across cell membrane • Increase plasma potassium; decreasing the resting membrane potential, increase excitability, muscle weakness • decreases the net difference between the cell’s resting potential and threshold (action) potential • Decrease extracellular potassium; decrease excitability M. Zaharna Clin. Chem. 2009
Potassium Role in Hydrogen Concentration • In hypokalemia (low serum K+), • As K+ is lost from the body, Na+ and H+ move into the cell. • The H+ concentration is, therefore, decreased in the ECF, resulting in alkalosis. M. Zaharna Clin. Chem. 2009
Regulation of potassium • The kidneys are important in the regulation of K+ balance. • Initially, the proximal tubules reabsorb nearly all the K+. • Then, under the influence of aldosterone, K+ is secreted into the urine in exchange for Na+ in both the distal tubules and the collecting ducts. • Thus, the distal tubule is the principal determinant of urinary K+ excretion. • Most individuals consume far more K+ than needed; the excess is excreted in the urine but may accumulate to toxic levels if renal failure occurs. M. Zaharna Clin. Chem. 2009
Hypokalemia • Decrease of serum potassium below 3.5 mmol/l Insulin promotes acute entry of K into skeletal muscle and liver by increasing Na, K-ATPase activity; Hypermineralocorticoid-like effects. In the kidney, cortisol activation of mineralocorticoid receptors alters renal tubular exchange of sodium (retained), potassium (excreted) M. Zaharna Clin. Chem. 2009
Hyperkalemia • Increase potassium serum levels > 5 mmol/l • Associated with diseases such as renal and metabolic acidosis M. Zaharna Clin. Chem. 2009
Potassium determination Assay method: • Ion selective Electrode • a valinomycin membrane is used to selectively bind K+ M. Zaharna Clin. Chem. 2009
Chloride • Major extracellular anion • Cl– is involved in maintaining: • osmolality, • blood volume, • and electric neutrality. • In most processes, Cl– ions shift secondarily to a movement of Na+ or HCO3–. • Cl– ingested in the diet is Completely absorbed by the intestinal tract. M. Zaharna Clin. Chem. 2009
Chloride • Cl– ions are filtered out by the glomerulus and passively reabsorbed, in Conjuction with Na, by the proximal tubules. • Excess Cl– is excreted in the urine and sweat • Excessive sweating stimulates aldosterone secretion, which acts on the sweat glands to Conserve Na+ and Cl– M. Zaharna Clin. Chem. 2009
Electric Neutrality • Sodium/chloride shift maintains equilibrium within the body. • Na reabsorbed with Cl in proximal tubules. • Chloride shift • In this process, carbon dioxide (CO2) generated by cellular metabolism within the tissue diffuses out into both the plasma and the red cell. • In the red cell, CO2 forms carbonic acid (H2CO3), which splits into H+ and HCO3- (bicarbonate). • Deoxyhemoglobin buffers H+, whereas the HCO3- diffuses out into the plasma and Cl- diffuses into the red cell to maintain the electric balance of the cell M. Zaharna Clin. Chem. 2009
Hypochloremia • Hypochloremia: < 98 mmol/l M. Zaharna Clin. Chem. 2009