Download
1 / 39
390 likes | 698 Views
Urinary Catheter-Related Infections and Infection Prevention Systems. Carol E. Chenoweth, M.D. Medical Director, Infection Control and Epidemiology. Prevention of Infections: “Bench to Bedside”.

E N D
Urinary Catheter-Related Infections and Infection Prevention Systems Carol E. Chenoweth, M.D. Medical Director, Infection Control and Epidemiology
Prevention of Infections:“Bench to Bedside” • Research findings “translated” into improved clinical care using the resources already in place at the UMHS • Infection Control and Epidemiology • UMHS Patient Safety Committee • Continuous Quality Improvement • Office of Clinical Affairs
Prevention of Infections • Prevention of urinary catheter infections • Prevention of central venous catheter infections • New methods of promoting hand hygiene
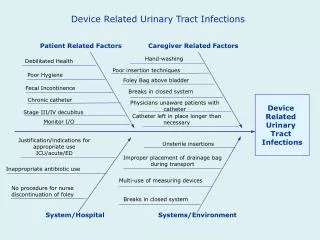
Urinary Catheter-related Infection: Background • Urinary tract infection (UTI) causes over 40% of hospital-acquired infections • Most infections due to urinary catheters • 25% of inpatients are catheterized • Leads to increased morbidity and costs
Prevention of Catheter-related Infection #1) Use a closed drainage system, aseptic placement and care #2) Make sure the catheter is indicated #3) Remove the catheter as soon as possible #4) Consider other methods for prevention
UTI Prevention Rule #2: Make Sure the Patient Really Needs the Catheter Appropriate indications • Bladder outlet obstruction • Incontinence and sacral wound • Urine output monitored • Patient’s request (end-of-life) • During or just after surgery (Wong and Hooton - CDC 1983) (Jain, Arch Int Med 1995)
Why are Catheters Used Inappropriately? • Perhaps physicians “forget” that their patient has a urinary catheter • Study to determine the extent to which physicians are aware which of their inpatients have urinary catheters • Surveyed 56 medical teams at 4 sites; 256 providers completed the survey (response rate = 89%) (Saint S, Wiese J, Amory J, et al. Am J Med 2000)
Urethral Catheters: Lost in Place? (Saint S, Wiese J, Amory J, et al. Am J Med 2000)
Systems Approach to Reducing Urethral Catheterization – U of M Medical Center • Funding provided by the Blue Cross Blue Shield of Michigan Foundation • Written reminder placed on the chart by a research nurse after 48 hours of catheter use • Before-and-after study on 2 hospital wards with 2 concurrent control wards • Data collection underway; also will evaluate UTI rates
Methods for Preventing Urinary Catheter-related Infection • Bladder irrigation: NOT • Antibacterial agents in collection bag: NOT • Rigorous meatal cleaning: NOT • Use of antiseptic urinary catheters
Prevention of Catheter-related UTI using Silver Catheters: The Silver Bullet? • Silver has in vitro antibacterial activity • Efficacy of silver catheters shown in meta-analysis of randomized trials (Saint, et al. Am J Med, 1998) • Additional cost of $5.30 per silver catheter tray • Is the reduction in catheter-related infection worth the extra cost?
Economic Evaluation of Silver Catheters • Decision analytic model comparing silver catheters with standard non-coated catheters • Patient population: hospitalized patients at high risk for infection requiring catheterization for 2 to 10 days
Results of base-case analysis: Silver catheters prevent morbidity and save money (Saint, Veenstra,, Sullivan, Chenoweth, Fendrick. Arch Intern Med 2000)
Silver Catheters: Policy Implications • Silver catheters should be considered in appropriate patients requiring catheterization for 2 to 10 days • Evaluate if silver catheters work at U-M
Catheter-related UTI Prevention:Summary Recommendations • Use only a closed drainage system and aseptic technique • Use urethral catheters only when necessary • Consider using an administrative catheter “stop order” to limit inappropriate catheterization • Consider silver catheters in high-risk patients who require catheterization for 2 to 10 days
Prevention of Infections • Prevention of urinary catheter infections • Prevention of central venous catheter infections • New methods of promoting hand hygiene
Catheter-related Bloodstream Infection (CR-BSI): Background • Vascular catheters are the leading cause of nosocomial bacteremia; most due to central venous catheters • 150,000 cases of CR-BSI annually in U.S. • 4% to 25% attributable mortality rate • Annual cost between $300 million and $2 billion
Prevention of Bloodstream Infections • Aseptic placement of CVC catheters • Antimicrobial catheters • Site disinfection
Full Barrier Protection for Insertion of CVCsRaad, Infection Control Hosp Epidemiol, 1994
Effect of Maximal Barrier Precautions during Insertion on CVC InfectionsRaad et al, Infect Control Hosp Epidemiol, 1994
Meta-analysis of Antiseptic Catheters: CR-BSI Tennenberg Maki Hannan Bach Heard Collin Ciresi Pemberton Ramsay Trazzera George OR 0.56, 95% CI (0.37-0.84) Summary 0.0 0.5 1.0 2.0 3.0 Odds Ratio (Veenstra, Saint, Saha, et al. JAMA 1999)
Economic Evaluation of Antiseptic Catheters • Is the benefit worth the extra $25 per catheter? • Decision model comparing antiseptic with standard catheters in patients at high-risk for CR-BSI (e.g. critically ill) using central lines for 2 to 10 days
Results: Antiseptic catheters saves money & lives (Veenstra etal, JAMA 1999)
Antiseptic Catheters: Implications • Antiseptic catheters recommended in critically ill patients requiring central venous access for 2 to 10 days • UM now using these catheters and recently evaluated the results
Which Disinfectant Should be Used for Catheter Site Care? • Povidone-iodine (PI) is currently the most widely used agent for site disinfection • Chlorhexidine gluconate (CHG) has been compared to PI with mixed results • We performed a formal meta-analysis of published and unpublished studies to clarify relative efficacy
Chlorhexidine for Site Disinfection: CR-BSI Favors CHG Favors P-I (Chaiyanupruk et al. Ann Intern Med 2002)
Which Disinfectant Should be Used for Catheter Site Care? Caveats • Chlorhexidine gluconate costs 2-fold more than povidone-iodine • $0.41 vs $0.92 for same amount • Effect of CHG in addition to antimicrobial catheters unclear • UM now using this new disinfectant and we plan to evaluate the results
Washing Hands to Stop Spread of DiseaseIgnaz Semmelweis (1818-1865) Handwashing is still the most important intervention to prevent health-care associated infections
Barriers to Handwashing ComplianceBoyce, Ann Intern Med, 1999 • Perceived or real time constraints • Skin irritation and dryness • Inconvenient locations of sinks • Lack of personal responsibility • Lack of awareness that hand hygiene effects clinical outcome
Antiseptic Hand Rinses • 60-70% alcohol solutions • Effective against most bacteria, viruses, fungi • Protective against hand drying • Faster, increased compliance
Effect of Hospital-Wide Hand HygienePittet, Lancet, 2000 Hand hygiene compliance Study times, 1994-97
Antiseptic Hand Rubs as Supplement to HandwashingSummary • Avoid if hands visibly soiled or contaminated with organic material • Increases compliance with hand hygiene • Decreases nosocomial infections? • Consider placement and dispenser carefully
Prevention of Infections Summary • Prevention of urinary tract infections • Decrease urinary catheterization • Administrative stop orders? • Antiseptic urinary catheters • Prevention of central venous catheters • Maximal barriers at placement • Antiseptic catheter • Chlorhexidine site disinfection • New approaches to hand hygiene