Download
1 / 32
330 likes | 1.15k Views
Considerations in Treating Individuals with Alzheimer's Disease From Hmong and Hispanic Cultures. March 24, 2007. Discussion Overview. Definitions Evercare and the people we serve Research Hmong Beliefs, Values and Preferences Hispanic Beliefs, Values and Preferences

E N D
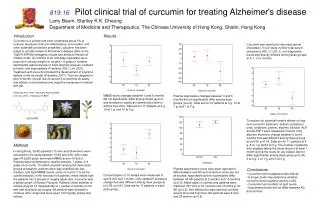
Considerations in Treating Individuals with Alzheimer's Disease From Hmong and Hispanic Cultures March 24, 2007
Discussion Overview • Definitions • Evercare and the people we serve • Research • Hmong Beliefs, Values and Preferences • Hispanic Beliefs, Values and Preferences • Key Clinical Issues in Treating Alzheimer's and Related Dementias (ADRD) • Caregiver Study • Case Discussions – Participants’ Experiences & Insights • Evercare Activities to Promote Clinician Cultural Proficiency 2
What is Multicultural Competence? • In General Terms: • Knowledge of various sets of personal/group attitudes, beliefs, values, communication, and behaviors that influence one’s interactive adaptation. This implies an awareness of differences and consistent application of this awareness • In Healthcare: • Practice of appropriate strategies and interventions based on that knowledge 3
Evercare and the People We Serve • Founded in 1987, headquartered in Minnetonka, MN • Division of Ovations, which is part of UnitedHealth Group • Largest national care coordination program nationwide • Serving >120,000 enrollees in Medicare and Medicaid plans in 38 states • Special Needs Plans: nursing homes, community-based (dually eligible, chronic illness Medicare-only, ESRD) • Plans through state Medicaid programs • Hospice & Palliative Care • More than 700,000 caregivers have access to special services via employer work-life programs Ethnically diverse enrollee base 4
Evercare – Who We Serve • 5+ chronic conditions = 2/3 of all Medicare costs • Great suffering & ineffective resource utilization • 50% of people die in hospital outside of Hospice • Poor palliation services • Maybe functioning well, but no reserve secondary to age • Sudden event is catastrophic • Single condition but very high impact, e.g. quadriplegia, advanced Alzheimer’s Disease 5
Evercare’s Approach • Clinical model focused on early detection of potential problems and individualized care. At its heart are Nurse Practitioners and Care Managers. • 500 Nurse Practitioners and 780 Care Managers • Individualized, holistic and “high-touch” approach to providing care management/care advocacy • Orchestrate services, effective integration of treatments, and better communication among enrollees, families, physicians and other health care providers • Continue to pilot innovative approaches designed to enhance health, well-being and functioning of members and families 6
Research • AD and Related Dementias • It is assumed that old-age dementia is present in all or nearly all populations • Literature on dementia in indigenous, traditional non-Western societies is scant • It is also assumed that it is likely to be experienced differently by different cultures • Prevalence is higher in Hispanic American populations than in Caucasians (2x as likely to develop by age 90 – Tang et. Al. JAGS 1999) • It is difficult to ascertain in the US Hmong population since so many died during their exodus from Laos 7
Research • Portion of elders who are white and non-Hispanic will decline from 87% (1990) to 67% (2050) • Demographics will drive cross cultural research on ADRD • Research challenges • Lack of culturally neutral and/or culturally fair cognitive tests, most research hasn’t considered degree of acculturation • Difficulty in evaluating years of education, quality of education and literacy • Despite limitations current research provides valuable information for clinicians treating individuals with ADRD from different ethno cultural groups 8
Hmong Culture, Preferences, Beliefs &Values • The Culture • One of the most homogenous cultural groups in our society • Hmong meaning & identity are linked to the family & clan (18 clans) • Needs of family are more important than those of an individual • Males are decision makers, and male clan leaders resolve disputes within clan, between clan & non-Hmong communities • Elders typically live with their eldest son • General Interactions • Address formally; Mr. & Mrs. Husband’s first name • Handshake with male, nod to female • No touching, hugging etc. by males & females in public • Eye contact is disrespectful • Females very modest & prefer female MD, if a male MD husband must be present 9
Hmong Culture, Preferences, Beliefs &Values • Religious Beliefs • Historically, Hmongs are animists; however a small percentage have become Christians • Animists believe that well being is dependent on harmony between the life & soul within the body & spirits outside the body • Animists believe that people are alive by chance & death takes place by chance • The Shaman is the key to communicating between the spirit world and human world • Health Beliefs • Pain and sickness are caused by imbalances in the spirit world • Spirit possession, soul loss, breach of taboo, physical injury or object intrusion are causes • Non-spirit illnesses can be seen externally & treated by folk practitioners or MD • Spirit illnesses can’t be seen & are treated by the Shaman 10
Hmong Culture, Preferences, Beliefs &Values • Beliefs Related to ADRD - Mary Olson research • We know that ADRD is a normal part of aging – not an illness • Hmongs believe that “Talking in tongues” (talking strangely, beyond death, hallucinations) is viewed as a mental illness (a source of shame) • Elders with ADRD are to be cared for by the eldest son or another son, if the son refused to do so they would be shunned by the community • Nursing Home placement is considered when the elder is very close to the end of life, although death at home is preferable • Decision to make requires all family members to be in agreement & may include the clan’s input • If a person is placed the family must come with Hmong food 3x day • Some Hmongs would allow placement of a nasogastric tube if the elder could no longer eat; others would not because of fear it would remain in the body after death resulting in reincarnation with the tube still in • Advance Directives are not common, end-of-life decisions are made by the family • It would be a disgrace to have the individual die alone in the Nursing Home 11
Hispanic Culture, Preferences, Beliefs & Values • The Culture • The Hispanic culture is not homogenous – there is a great deal of ethnic diversity within the culture • Acculturation varies greatly among the US Hispanic population • Hispanic cultures are usually patriarchal with males making the majority of the decisions; however the females tend to make the day-to-day health care decisions • The family is more important than the individual, and family self-reliance is key • General Interaction • Hispanics often carry the father’s & mother’s last name • Recent immigrants avoid eye contact with individuals as a sign of respect • Physical touch and warm smiles are preferable to handshakes (too formal) • Anyone working with family is expected to invest time getting to know them • Time is very flexible & being late is acceptable 12
Hispanic Culture, Preferences, Beliefs & Values • Religious Beliefs • Catholicism is the dominant religion; however a small percentage are Protestant or Jewish • Belief in an after life is common among Hispanic individuals who are Christian • Health Beliefs • There is a great deal of variance in beliefs about the causes of illness • Some believe that God determines the outcome and that prayer is the best response • Some believe that negative behavior is the cause of illness • Others believe illness is associated with an imbalance between nature and the supernatural • HIV/AIDS, alcoholism and mental illness carry strong stigmas for many 13
Hispanic Culture, Preferences, Beliefs & Values • Beliefs Related to ADRD – from the Hispanic point of view (unless otherwise noted) • Mental Illnesses or negative emotions featuring stress, genes, trauma, nutrition, aging and brain deterioration are all seen as causes of ADRD • Memory impairment is considered a normal part of aging • Diligent caregiving can control or prevent behavioral disturbances and further memory impairment • Dementia is often viewed as a mental illness & source of shame • Family secrets including shame shouldn’t be shared • Caregiving of an elder with ADRD is typically provided by a daughter • Mexican Americans may associate ADRD with shame and avoid seeking services (Gallagher-Thompson study) • If ADRD is viewed as the will of God or the “evil eye” - care may not be sought • Extended family makes end of life decisions – death at home is preferred • Advance Directives are not common 14
Clinical Areas for Interactions with Patients & Families • Mental status or cognitive changes are often first recognized by family members • Delirium often misdiagnosed/undetected • There are reversible causes of dementia that can be treated • Early comprehensive clinical evaluation essential • Recognize and treat depression results in improved dementia outcomes • Ongoing patient assessment is important to provide quality of care, maximize functional performance by improving cognition, mood, and behavior • Ongoing medical/cognitive assessment • Preventive care, early recognition of changes in condition • Caregiver training vital • Planning for future needs critical 15
Evercare Study of Caregivers in Decline • 44 million Americans are caregivers for their loved ones; more than 21% of U.S. households contain at least one family caregiver • 2004 National Alliance for Caregiving and AARP Study: 2.5 million caregivers in fair or poor health • The role of the caregiver runs through all of Evercare’s offerings • Important to find out why their health was declining and what solutions there are to help • Collaborated with the National Alliance for Caregiving • Result: first survey to take a comprehensive look at the impact of caregiving on the health and wellness of caregivers 16
The Headline… • Stress and worry of caregiving leads to: • Depression • 91% reported they suffer from depression • 81% said caregiving made their depression worse • Extreme fatigue • Poor eating and exercise habits • Greater use of medications • Misuse of alcohol or prescription drugs to cope • 53% said this “downward health spiral” also negatively affects their ability to provide care If caregivers become too ill to care for their loved one, we have a growing public health issue as our population ages 18
What Can Help? % Very/somewhatlikely to use 19
Clinical Areas for Interactions with Patients & Families • Behavioral disturbance occurs in >50% of people with dementia - agitation, aggression, pacing, wandering, mood disturbances, personality changes, changed sexual behaviors, decreased appetite & psychosis • Stressful for caregivers/ families, great burden • Rule out potential medical causes (UTI, Pain) • Effective interventions exist: behavioral, environmental, and pharmacologic • Identifying triggers for behaviors is important • Ideal environment is familiar, constant, and non-stressful • Train caregivers on successful approaches for behavior 20
Clinical Areas for Interactions with Patients & Families • ADRD behavioral disturbances impact activities of daily living (ADL) • Families/caregivers need to understand prognosis, expect decline in self care of ADLs • Planning for future care needs is critical • Eating and drinking: seen in 92% of patients with dementia, review potential causes and potential strategies to intervene • Toileting: incontinence and constipation common • Bathing and hygiene problems: common, use person-centered strategies to resolve • Gait disturbances: common in advanced stages of dementia 21
Case Discussion What is Your Experience With ADRD in Hmong and Hispanic Cultures? • Has your experience validated the “Culture, Preferences and Beliefs” for the Hmong & Hispanic populations presented today? • What were some challenges dealing with these beliefs and preferences? • How did you use your understanding of the Hmong & Hispanic culture in each of the clinical areas mentioned today? • Are some issues more cultural-dependent than others? • How did/do you learn about the cultures of the patients you treat? 22
Evercare: Addressing Diversity in Daily Practice • Outcome of advisory council info: • Selected top 3-5 actionable items that would help our clinician communicate and serve our diverse customers’ unique needs • Action items appear on the Plan of Care, for example, if our client was of Hmong background, we would consider the following: 23
Evercare: Online learning mandatory for all staff • Online course with activities and post-test. • More than 1,500 employees have completed the course. 24
Online Course Content: Cultures & Topics • Targets most commonly occurring diverse populations. • Addresses some background about general beliefs, health disparities, and health/ illness/end-of-life beliefs. 25
Addressing Linguistic Competency • Educated field on how to access phone interpreters via use of dual handset phones • Sites order phones directly through contracted vendor for OPI (Over the Phone Interpretation) • Call centers use contracted vendor for on-the-spot translations to complete assessments and conduct care management activities • Customer Service and Sales Call Centers equipped to translate calls in 20+ languages 26
Culture and End-of-Life Care: All Clinicians • Purchased interactive training program to train clinicians on cultural considerations when planning/managing end of life care 27
Albanian Native American African Portuguese Cape Verdeen Russian Chinese Somali Haitian Spanish Hmong Taiwanese Korean Vietnamese Muslim (Arabic) Cultural Advisory Groups • Contracted with Language Services Inc. to develop 15 advisory groups using medical translation experts Focus groups gathered to discuss 11 major topics about cultural beliefs about health, illness, end-of-life. Final product: 70+ page advisory report with tips for communicating and caring for people of diversity. 28
FiveWishes®: Advance Care Directives in 20 Languages • NEW INITIATIVE UNDER WAY TO PROVIDE ADVANCE CARE DIRECTIVES • TO ETHNICALLY AND CULTURALLY DIVERSE COMMUNITIES • End-of-life decision-making program translated into 20 languages • Outreach in 38 states through communities, hospitals and hospices • Eliminates barriers to end-of-life decision-making for non-English-speaking members of ethnically and culturally diverse communities 29
Evercare University Intranet Site • Communicating cultural tools, resources and updates to our clinicians via our intranet site: 30
Evercare Internet Site For more information on products and services offered by Evercare, please visit: www.EvercareHealthPlans.com Coming in Summer 2007: The launch of our new Spanish website – www.PlanesDeSalud.com-- a website incorporating the unique needs and culture of our Hispanic populations. 31