Download
1 / 14
140 likes | 151 Views
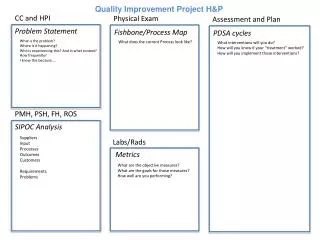
This project aims to improve the efficiency and quality of care for children with Congenital Heart Surgery (CHS) by implementing Prevention Infection Bundles (PIB) in the postoperative recovery unit. The objective is to decrease infection rates and reduce morbidity and mortality among children with CHS.

E N D
Develop a QualityImprovementImplementation Project “Health Team Quality Improvement Implementation Project and the Impact upon Congenital Heart Surgery Infection Rate” Bustamante P RN, Perez Ferrero J RN, Rodriguez R RN, Benedetto E RN, Oyola D RN, Juaneda I MD, Juaneda E MD.
Local Problem • CICU at HNST semiannual unadjusted infection rate: 24% and23% at 2012; 26% and 14% during 2013 and 14% on 2014. • Data infection rate are higher than 4-6% IQIC participants.
StudyQuestion • Is it possible to reduce unadjusted infection rate through Prevention Infection Bundles (PIB) implementation on CHS postoperative recovery in the CICU at HNST ?
Objetives • Health Team: Incorporate patient's safety culture, improving efficiency and quality of care of children with Congenital Heart Surgery (CHS) and assess if through to quality improvement project decreased infection rates on CHS. • Patients: To decrease morbidityand mortality in children with CHS.
Methods • A quantitative, correlational and prospective study. • Postoperatory of CHS in children’s from 0 - 14 years of age between January1st 2014 to December 31st 2015.
StudyStages Stages: • Staff Capacitation and Strategy Orientation • Strategy Implementation • Monitoring Implementation • Data quantification and analysis • Changes implemented by the analysis
Analysis and Evaluation • Specific Prevention Infection Bundles (Daily-Checklist for NAV, CVL, SSIs and UTI) rate adherence according score 0-Incompleted, 1-Completed, unadjusted infection rate provided by IQIC and correlation statistics analysis between both.
Parcial Results January 2015 CVC May 2015 CVC
Parcial Results January 2015 VAP May 2015 VAP
Parcial Results January 2015 UTI May 2015 UTI
Challenges • Obtain the 80% percentage adhesion to the Prevention Infection Bundles • Implement new strategiesrelatedto Safety patient, control infection and teamwork • Showingstatisticsmonthly • Developedstaff training in SimulatedPracticeLab.
References • Richardson W et al. CrossingtheQualityChasm: A New HealthSystemforthe 21st Century (Free executivesummary) http://www.nap.edu/catalog/10027.html • Linda T. Kohn, Janet M. Corrigan, and Molla S. Donaldson. ToErrIsHuman: Building a SaferSystem, Editors; ComitteeonQuality of HealthCare in America, Institute of Medicine; NationalAcademyPress 2000. • Bode, L. 2010). PreventingSurgical-SiteInfections in Nasal Carriers of StaphylococcusAureus. The New EnglandJournal of Medicine. • Guardia et al. 2008). InfeccionNosocomial en Postoperados de Cirugia Cardiaca. Anales de Pediatria., http://analesdepediatria.org/es/infeccion-nosocomial-postoperados-cirugia-cardiaca/articulo/S1695403308702352/. • Ministerio de Salud de la Nacion Secretaria de Politicas, R.e. (2011). Reporte Semestral Enero-Junio 2010. Programa Nacional VIDHA. Obtenido de www.vihda.gov.ar • Hales, M.a. (2006) TheChecklist – a Toolfor Error Management and PerfomanceImprovement. Journal of CriticalCare, http://www.jccjournal.org/article/S0883-9441(06)0081-5/abstract#. • Weiser. T et al. (2010) Perspectives in Quality: Designingthe WHO Surgical Safety Checklist. International JournalforQuality in HealthCare. http://intqhc.oxfordjournals.org/content/22/5/365.article-info. • International QualityImprovementCollaborativeforCongenitalHeartSurgery in DevelopingCountries. Annual Data Report 2012,2013,2014. Hospital de Niños – Cordoba-Argentina.