Download
1 / 30
310 likes | 431 Views
Detailed overview of venous reconstruction during cancer surgery involving major veins, challenges for vascular surgeons, methods, and conduits used for reconstruction. Includes case studies and alternative methods for size matching in reconstruction.

E N D
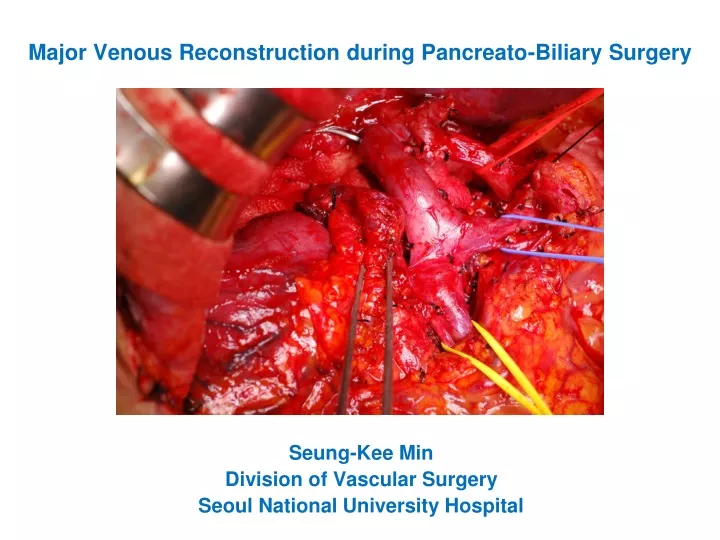
Major Venous Reconstruction during Pancreato-Biliary Surgery Seung-Kee Min Division of Vascular Surgery Seoul National University Hospital
Cancer invasion to major veins during HBP surgery • Inferior vena cava, portal vein, or superior mesenteric vein • Venous reconstruction is required for complete resection. • A challenge for a vascular surgeon • Size mismatch • Lack of suitable autogenous conduit • Risk of infection
Methods of PV reconstruction (1) • End-to-End anastomosis • Patch angioplasty 3. Interposition graft No tension ! No stricture !
Methods of PV reconstruction (2) • End-to-End anastomosis • Patch angioplasty 3. Interposition graft Lee et al. J Vasc Surg (2010)
Methods of PV reconstruction (3) • End-to-End anastomosis • Patch angioplasty 3. Interposition graft Lee et al. J Vasc Surg (2010)
Conduits for PV reconstruction 1. Autogenous vein • Femoral vein (SFV) • Left renal vein • Internal jugular vein • GSV • Gonadal vein 2. Homograft ; Cadaveric iliac vein (risk of degeneration and chronic rejection) 3. Bovine pericardium 4. Prosthetic graft ; ePTFE, Dacron (risk of infection) 5. Autogenous peritoneum (anecdotal use)
Case 1. Pancreas cancer with PV/SMV invasion • Bovine patch angioplasty
Case 2. Pancreas cancer with PV/SMV invasion • Patch angioplasty with bovine pericardium Portal vein Splenic vein IVC Bovine patch Lt. RV Rt. RV SMV
Case 3. Pancreas cancer with SMV invasion • interposition graft with bovine pericardium
Case 4. Pancreas cancer with SMV invasion • interposition graft with bovine pericardium
Case 5. SMV Reconstruction with spiral graft • F/68, pancreatic cancer • CT: a mass at uncinate process of pancreas with SMV invasion
Operation • PPPD • Segmental resection of PV/SMV & interposition graft with GSV • Small bowel edema due to size mismatch • PTFE interposition graft (10mm) • 2 days later, second-look operation was done • Total occlusion of PTFE graft Chiu et al. Vasc Endovasc Surg (2007)
Spiral graft with GSV • To overcome the size mismatch & infection Chiu et al. Vasc Endovasc Surg (2007)
Reconstruction with spiral vein graft v PV Spiral vein recon. SMV SMA SMV
Follow-up CT scan Patent spiral graft at postoperative 3 months
Spiral vein graft • Harvest of saphenous vein -- from groin to calf or ankle -- Length (D) = radius (R) / radius (D) x length (R) • Advantages -- can be tailored to fit a vessel of any size -- ease of handling and superficial dissection -- large vessel substitute without the drawbacks of prosthetic graft • Indications -- Major visceral vein reconstruction -- IJV reconstruction after RND -- Mesocaval shunts in children -- replacement of CFV after trauma -- After removal of infected prosthetic graft -- Axillary, subclavian or femoral artery reconstructions
Other methods for size matching Yamamoto et al. Langenbecks Arch Surg 2009
Case 6. Pancreas cancer with SMV & HA invasion • Portal vein; End-to-end anastomosis • Hepatic artery; interposition graft with GSV
Complicated cases * Reconstructed later by spiral GSV graft Kim SM et al. J Korean Surg Soc 2013;84:346-52
The fate of portal vein occlusion • Extrahepatic portal vein occlusion • Anomaly in children • After biliary operation in children • Portal vein invasion of malignancy • Pancreatic cancer • Colorectal cancer with liver metastasis • After liver transplantation Variceal bleeding from the Hepatico-Jejunostomy
Intervention first, but not always possible Transhepatic or transsplenic Portal vein stent-graft H-J Varix embolization
Rex shunt, revisited • Bypass between SMV-Lt portal vein in Rex recessus (umbilical fissure along umbilical vein in round ligament between segment III & IV) • Most physiologic • Limitation by the left PV status • Surgery of choice in extrahepatic portal vein occlusion, especially in children • Remained hepatopedal flow ; avoiding hepatic atrophy • No porto-systemic shunt ; minimizing hepatic encephalopathy • Conduit; autogenous vien – IJV, both GSV (1st done in 1992 , de Goyet, for EHPVO after LTPL)
Meso-Rex shunt Meso-Rex shunt with transposed coronary vein Cho YP et al. ASTR 2014
Take-home messages • Methods of PV reconstruction ; primary repair, patch angioplasty & interposition graft ; No tension & No stricture ! • Conduits of PV reconstruction ; autogenous vein ; tailored vein graft -- spiral graft ; bovine patch, cryopreserved vein, synthetic graft • Long-term fate of PV occlusion may result in fatal variceal bleeding from the hepatico-jejunostomy site.