Download
1 / 31
320 likes | 663 Views
Community Care of North Carolina . Child Health Accountable Care Collaborative (CHACC). Key Goals. Improve access to, quality of, and coordination of care By doing so, decrease the cost of care. Community Care of NC. Statewide primary care medical home & care management system

E N D
Community Care of North Carolina Child Health Accountable Care Collaborative (CHACC)
Key Goals • Improve access to, quality of, and coordination of care • By doing so, decrease the cost of care.
Community Care of NC • Statewide primary care medical home & care management system • Rests on foundation of Carolina Access Medicaid in which Medicaid patients are linked to a primary care home • Provides resources to improve access to, quality of and coordination of care across the different segments of the local health care system and decrease cost of care • Private-public partnership (all savings stay in NC) • Provides ready access to data • Community based, locally driven, provider led
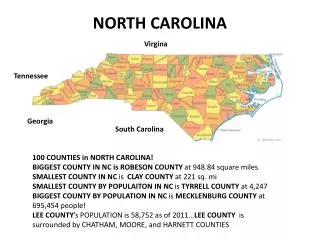
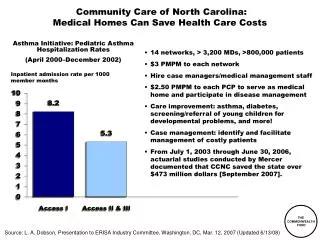
Local Networks • 14 local Networks across all 100 NC counties with more than 4500 Primary Care Physicians (1360 medical homes) • Over 1.4 million Medicaid enrollees, including dual Medicare/Medicaid and Health Choice enrollees
Local Networks • Are non-profit organizations • Provide resources to primary care homes to better manage Medicaid population • Join public and private sector primary care homes with other segments of the health care system (e.g. hospitals, health departments, mental health agencies, social services) to create local systems of care • Utilize local multi-disciplinary RN and SW care managers, pharmacists, psychiatrists, obstetricians, medical directors • Pilot potential solutions, share best practices • Are capable of and accountable for managing recipient care
Main Program Activities • Chronic Disease Management Initiatives (e.g. Asthma, Diabetes) • Chronic Care Initiative • Hospital Transition Care • Quality Improvement Initiatives • Emergency Department Utilization • Chronic Pain Initiative • Integration of Physical and Mental Health • Prevention Initiatives • Pharmacy Initiatives • Palliative Care • Access to Primary Care • Support of IT Initiatives • High Risk Pregnancy Care Management
Key program Asset- Access to dataInformatics Center • Medicaid claims data • Utilization (ED, Hospitalizations) • Providers (Primary Care, Mental Health, Specialists) • Diagnoses • Medications • Labs • Costs • Individual and Population Level Care Alerts • Reports on high-opportunity patients • Quality Measurement and Feedback Review System
Key program Asset- Access to dataReal Time Data • Hospitalizations • ED visits • Provider Referrals
Link to local health care system and community resources Multidisciplinary management support QI Support Primary Care Home Patient
Public Health Hospital Behavioral Health Primary Care Home Patient ~Specialists~ Community Resources Social Services
Child Health Accountable Care Collaborative (CHACC) CMS Innovations Project Partnership of Community Care of North Carolina and Children’s Health Care Providers
CHACC • 3 year Cooperative Agreement from the CMS Innovations Center to Community Care of North Carolina--July 1, 2012- June 1, 2015 • Partnership of CCNC with Children’s Primary Care and Specialty Care Providers; and the Academic Medical Centers and Children’s Tertiary Care Hospitals to improve the health of NC children who have complex and chronic illness
Child Health Accountable Care Collaborative (CHACC) • Partnership with North Carolina’s Children’s Healthcare Providers, North Carolina’s Academic Medical Centers and Tertiary Medical Centers Community Care of North Carolina CHACC Project Director Steve Wegner, MD Medical Directors Elizabeth Tilson, MD (CCNC Networks) David Tayloe, MD (Primary Care) Alan Stiles, MD (Pediatric Subspecialists/Hospitals) CHACC Integration Workgroup Program Director Sherri Branski, RN, MSN, CCM Lynn Guerrant, RN, MS CCNC Networks/Primary Care Providers Medical Home CCNC Network Care Managers Pediatric Subspecialists/AMCs/Tertiary Children’s Hospitals CHACC Lead Care Managers, Care Managers, and Patient Coordinators
Program Goals • Improve the health of NC children with complex chronic illnesses through improved value of care. • Engage primary care providers and pediatric subspecialists across the state to share responsibility and accountability for pediatric primary, subspecialty, and hospital care. • Jointly develop and utilize evidence based guidelines of care for pediatric chronic illnesses with pediatric subspecialists and primary care physicians and actively engage in co-management of these children. • Provide active care management to children under the care of pediatric subspecialists through embedded care managers and patient coordinators at tertiary hospitals and provide a warm hand off to CCNC network care managers.
CHACC Children with complex, chronic Illnesses Primary Care Specialty Care CCNC Networks--Medical Home/Primary Care Providers Pediatric Subspecialists/AMCs/Tertiary Children’s Hospitals CCNC Care Managers Co-management CHACC Care Manager Patient Coordinators
Cost Savings Approaches • Reduce hospitalizations through co-management and active monitoring of disease processes • Improve primary and preventive care for children with chronic illnesses by providing this care in a medical home • Reduce utilization of emergency services and pediatric subspecialists for acute common illnesses for these children • Reduce duplication of laboratory and medical studies through streamlined communication between primary care providers and pediatric subspecialists • Reduce pharmacy costs through formulary utilization and evidence based care
Timeline • Operations plan submitted to CMS, August 8, 2012 • Anticipate CMS approval by September 10, 2012 • Convene a CHACC Integration Workgroup August 2012 • Information sessions and discussion at the NC Pediatric Society Meeting September 2012 • Refine target population for intervention August to December, 2012 • Hiring and training of care managers and patient coordinators September 2012 to January 2013 • September 2012 to June 2013 Consensus Sessions of PCPs and Subspecialists
The Role of the General Pediatrician David T. Tayloe, Jr., MD, FAAP
Children and Youth with Special Health Care Needs (CYSHCN) • Registry of Patients • Care Plans • Subspecialist Care Coordination • Primary Care Physician Care Coordination • Community Partners • Family Involvement
Goldsboro Pediatrics • 15 pediatricians, 7 nurse practitioners, a physician assistant, 2 behavioral health professionals, 1 lactation consultant • 4 offices serving children in 7 counties • Electronic Health Record System • 2 Community Care of NC AccessCare staff • Community Hospital with Level 2 Neonatal Unit
Innovative Approaches • Children and Youth with Special Health Care Needs in Wayne County • Steering Committee of Family Members of CYSHCN and Community Partners • Goldsboro Pediatrics electronic health record system (secure intranet) • Registry and HIPAA-compliant /FERPA-compliant family consent procedures
Wayne Pediatric CME Series • Category I CME Sessions co-sponsored by the Office of CME at the Brody School of Medicine and Goldsboro Pediatrics • Meets at 7 AM in the private dining area of the hospital cafeteria most every Tuesday morning • Community Partners invited to attend sessions
Wayne Initiative for School Health (WISH) • Goldsboro Pediatrics is the medical home for the students enrolled in the six school-based health centers of WISH • Nurse Practitioner and Physician Assistant, with the help of RN’s, clerical staff, Registered Dietitians, behavioral health professionals provide comprehensive care for many at-risk middle/high school students in Wayne County
Community Care of NC • Care Coordinator and Patient Navigator are based in the main office of Goldsboro Pediatrics • CCNC staff attend CME sessions of the Wayne Pediatric CME Series • CCNC staff work closely with Community Partners
4% of Children • Need continuous care by pediatric subspecialists • Should have care plans/passports developed by their subspecialist teams • Need multiple services at the community level • Need 24/7 access to a physician who has access to the medical records of the child
Quality of Care for Children with Complex Medical Conditions • Guidelines and care plans/passports developed by subspecialists • Electronic communication involving tertiary center specialists and community based generalists • Regular visits with subspecialists and primary care physicians • Family input/electronic communication with physicians • Community partner collaboration coordinated by the community-based medical home
Cost-effectiveness of Care for Children with Complex Conditions • 24/7 access to subspecialist and generalist physicians • Avoid unnecessary expensive medications and therapies • Avoid unnecessary hospital emergency department visits • Avoid unnecessary hospital admissions
Shortage of Pediatric Subspecialists • Complex children need a lot of time from their pediatric subspecialists • NC has shortages of most categories of pediatric subspecialists • If these subspecialists are to maximize their time with complex children, general pediatricians must do their part to minimize unnecessary referrals to subspecialists
David T. Tayloe, Jr., MD, FAAP • Goldsboro Pediatrics 2706 Medical Office Place Goldsboro, NC 27534 919-734-4736 fax 919-580-1017 dtayloe@aap.org
“The project described was supported by Funding Opportunity Number CMS-1C1-12-0001 from Centers for Medicare and Medicaid Services, Center for Medicare and Medicaid Innovation.” “Its contents are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies.”