Download
1 / 38
380 likes | 655 Views
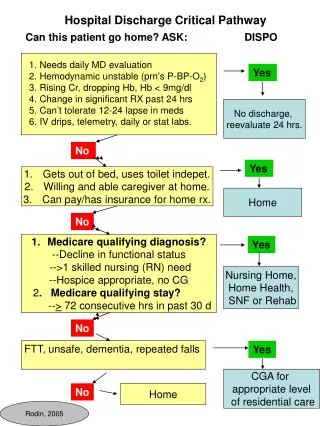
KANGAROO OTHER CARE METHOD. In- hospital Kangaroo adaptation and Discharge policies Module 4. KMC Components. 1 st : Kangaroo position The infant is placed almost naked in strict upright ventral position between the mother´s breast, in direct contact with her skin, as long as possible

E N D
KANGAROO OTHER CARE METHOD In- hospital Kangaroo adaptation and Discharge policies Module 4
KMC Components • 1st : Kangaroo position • The infant is placed almost naked in strict upright ventral position between the mother´s breast, in direct contact with her skin, as long as possible • 2nd : Kangaroo Feeding and Nutrition strategy • Ideally exclusive breastfeeding to have a weight gain similar to the growth during the intra uterine life (15 g/Kg/day )until full term • 3rd : Early Discharge and strict ambulatory follow up • Discharge in kangaroo position regardless of weight and gestational age when the child is able to coordinate sucking, swallowing and breathing , gaining weight for 3 days and have parents informed , trained and ready to come to follow up visits
Definition of Kangaroo adaptation • The Kangaroo Adaptation it is the process by which the responsibility to care for their preterm or LBW infants is gradually transferred from the heath team to the parents • Kangaroo adaptation is an indispensable step for the success of KMC • It refers to the social, emotional and physical adjustment of the mother and family of the preterm and/or LBW to the Kangaroo Mother Care Method. • It is the gradual and systematic training process of the child’s mother and family in the Kangaroo Mother Care Method.
Beginning of the hospital KMC adaptation • The process must begin as soon as possible, at birth, if the health of infant and mother allow it • Often the physical contact and, particularly the kangaroo position, begins: • When the child has successfully completed the immediate and intermediate adaptation to extra uterine life • When the child is physiologically stable enough to be manipulated • The process of adaptation starts by the assessment of the tolerance to the kangaroo position of both mother and infant. • Sessions in Kangaroo position are progressively prolonged until 24 hours kangaroo position is achieved • The process continues until the child is discharged from the Neonatal Unit in kangaroo position to ambulatory follow up
Rational for in hospital KMC adaptation KMC adaptation is achieved through a clear and comprehensive didactic process together with a strong emotional and social support • KMC adaptation is a well-planned process to help the mother/caregiver of the preterm infant • To overcome the stress due to the manipulation of the small infant • To facilitate nursing • To generate skill and confidence in caring for him • To be informed of the normal characteristics of a preterm infant • To be aware of the precautions to use • To be fully informed on the alarm/danger signs • KMC adaptation is a team work where a the role of a professional nurse is crucial she needs • with significant experience on breastfeeding, • good understanding of stress management • adaptive mechanisms • The psychologist plays an important role supporting the emotional crises of parents facing the preterm birth and the hospitalization of their infant
Steps of Kangaroo adaptation (1) Use of a standardized protocol based on scientific evidences for adaptation and implementation of the kangaroo position to maximize the benefits for children and parents and to limit the risks • Information of mothers/parents: It is fundamental to prepare parents, especially mothers before implementing the KMC • If risk of preterm delivery the benefits of the position must be repeated to motivate the mother to be with her child as much possible • All practical aspects of visits or prolonged/permanent stay during the child’s hospitalization should be explain to parents
Steps of Kangaroo adaptation (1) Use of a standardized protocol based on scientific evidences for adaptation and implementation of the kangaroo position to maximize the benefits for children and parents and to limit the risks 2.Identification of beneficiary dyads mother-infant to KMC: A member of the team usually a nurse, identify, at an early time, the infants who could benefit from the kangaroo position • Often the 1stfirst important step for parent in kangaroo adaptation is to visit their newborn infant in the Neonatal Unit and to stay near to him The mother is the ideal and main provider but if she is unavailable, the father or any family member can immediately begin the kangaroo position
Implementation of Kangaroo Position (2) 3.Assessment of clinical status of infant and mother : the situation of infant and mother must be evaluated to decide to begin the KP • The ideal is to begin as soon as possible, if the baby is close to term and the mother is alert, KP starts in the delivery room 4.Adequate clothes for mother and infant • Mother/kangaroo provider must wear clothes with frontal access • A support system must be provided in order to hold the baby(Lycra™ girdle or band) • The infant should be naked except a cap ( wool or cotton) , a sleeveless cotton shirt open in the front, socks and a diaper
Implementation of Kangaroo Position (2) 5. Placing the infant in Kangaroo position requires trained staff • The mother must hold him by placing one hand on the neck and back, with her fingers under his chin, the other hand is placed under the baby’s buttocks • The kangaroo baby is in upright position and ventral decubitus, with his body and head against the mother’s chest, in a” frog-like position” 6. Maintaining Kangaroo position and feeding • The kangaroo baby must always be kept in kangaroo position, safe for diaper change and breast feeding • Breastfeeding should be initiate as soon as possible • During breastfeeding, the lateral position is recommended allowing skin-to-skin contact • The child should be in skin-to-skin contact, ideally 24 /24 hours • The kangaroo provider must sleep in a reclined position, of at least 30º
Implementation of Kangaroo position (3) 7. Monitoring the adaptation to the kangaroo position for infant and mother to maintain or to interrupt it • Assess the baby for the regularity of breathing, state of alertness, color, general aspect, posture, apparent comfort or discomfort, sleep and alert periods in kangaroo position • Assess the mother’s attitudes, tolerance and emotional state • Monitoring of adaptation of the kangaroo provider-child dyad must be done by a trained staff under the supervision of the pediatrician
Aims of in-hospital kangaroo adaptation • Train mother/ family to care for the preterm following the KMC guidelines • Decrease the mother’s anxiety and build her confidence caring for her child • Promote bonding between mother and infant • Develop the mother’s skill in breastfeeding • Assess the child’s ability to suckle, swallow and breathe • Identify and build on the individual/ familial strengths in caring for the child • Help parents identify support systems and networks before the child’s home coming • Collaborate with families in the planning and provision of care for the child at home • Answer questions and address concerns of parents on KMC • Help the parents achieve the adaptation tasks related to feeding, recognizing danger/alarm signs and behavioral characteristics of the preterm child
Emotional support to families during in- hospital KMC adaptation • Premature birth , causes a disruption of the normal emotional adjustment to gestation and impairs the normal and healthy bonding process • The real suffering begins after delivery, when parents lose hope to have a healthy child • 77% of mother feel guilt and helplessness in the face of their child’s prematurity, perceived as small, and deformed • When the child is discharged from the Neonatal Units parents usually debate between different emotional states: • fear of taking the child home, • exhaustion from the daily work carried out in the neonatal unit • some confusion about the changes the family faced during the hospitalization of the preterm child
Emotional support to mothers The emotional support provided to the mother during the kangaroo adaptation must help her to cope with her fears about her capacity to care and breastfeed her child • Approach the mother in an empathic manner • Call the mother and her child by their names • Allow the mother to express her fears and concerns • Help the mother understand and interpret her feelings at the beginning of the adaptation • Talk without raising the voice, using a warm and friendly attitude • Establish eye and physical contact, as culturally appropriate • Promote a positive attitude in the mother, reassuring her in her achievements and making her feel proud of her motherhood • Respect the unique physical and psychological pattern of every mother
Involvement of fathers in KMCand emotional support • The role of fathers is determined by culture and society • KMC stimulates the early and active participation of the father and increases his responsibility and competence to care for and raise his child • In KMC fathers experience early attachment : • Skin-to-skin contact with their child is a positive experience • The kangaroo position favors the father’s sensitivity, and changes his perception of his fathering role • Fathers must have extensive and early exposure to their babies in the hospital • Provide guidance to the father to care for his child • Fathers need, just as mothers do, encouragement and support to adapt to the situation
In hospital adaptation activities • Organize parent support groups where they can freely express their concerns, fears and coping strategies. Within this space, parents can also be helped to re-define their roles and family relations • Integrate the mother/father to other educational activities and experiences : • To enable parents to gain confidence to care for the child, • To implement the KMC • To be prepared for discharge • Ideally, these sessions can be conducted at least twice a day • One session should be organized on recognizing fears and concerns before the discharge • to bring out and face any fears and concerns; discuss them and find ways to solve them
Relaxation technique for mothers Relaxation will help the mother to feel rested, decreasing the tension generated by holding and nursing the child The mother must be seated in a comfortable chair, with a footrest , with the child in kangaroo position inside the girdle • Indicate to the mother how to take deep breaths, inflating the abdomen and slowly breathing out 2. Show how to relax different parts of the body while breathing • Ask the mother to perform exercises of different part of the body 3 or 4 times, while breathing • Show how to alternate lifting and lowering shoulders with breathing • Then ask her to listen to her own breathing pattern and to become aware of her own body • Ask to mother to feel her own baby’s respiratory rate on her chest. • After a few minutes of rest, ask the mother to observe her child and share her experience with other mothers, if she is willing.
Visualization of home care • An effective way to explain to the mother what it will be to care for her baby at home is to invite one of the mothers from the ambulatory program: • to comment on her experience • to answer questions from the mothers who are in the adaptation process of KMC • Some questions may be formulated to be discussed • What was your main concern before discharge with your baby in kangaroo position? • As a mother, what is the most positive thing you felt when holding your baby in kangaroo position? • What has been the most difficult thing in this process and how did you manage it? • How has your child progressed since he was discharged and what are the benefits of taking him to ambulatory consultation?
Characteristics of preterm infants • The concept of “corrected age” must be explained to parents as the development of their child will be evaluated it • Corrected age is calculated by subtracting the number of weeks needed to reach 40 weeks of gestation, from the weeks passed since birth. • The characteristics of preterm infants must be explained to parents • They are conversant with these characteristics and will understand the changes they will observe in time • Some of these characteristics are shown below
Care and precautions for home care The infant should not be bathed until he reaches 40 weeks of GA. • Baby hygiene:The ‘kangaroo’ child’s basic hygiene is focused on the diaper change : the change must be performed • every time there is a need to change a soiled or wet diaper • in a place free of drafts , easy to clean • In an area where the baby can be placed, lying down on a tilted surface, 20-30º to avoid reflux and bronco aspiration • Wash hands before and after changing the baby • Prepare all equipment: a diaper of appropriate size, wet wipes , cream and cotton if prescribed • Carefully remove the tapes of the diaper and assess the child’ skin • Wipe the perianal area with a wet piece of cotton, from the inside to the outside, turning the child gently on his side. Never tilt the legs or hips above the level of the thorax to avoid reflux, bronco aspiration and increasing intra cranial pressure • Dry the skin with a piece of soft tissue or dry cotton. • Place a clean diaper, making sure that the umbilical stump is not inside the diaper. • Place the child in kangaroo position again. • Collect and discard the materials used
Care of the umbilical cord/stump • If there still an umbilical stump when the child is discharged, parents must be shown how to clean it • This area must be carefully disinfected to prevent infection • wash hands with soap and water • use 1 or 2 cotton swabs, moistened in an antiseptic solution. • The stump is lifted to clean its base with the swabs • Insure that the cord/stump is not inside of the diaper • Wash hand again and discard the use cotton swabs • If the umbilicus is red, swelling or draining pus refer immediately to hospital
Others home care Cleaning the nose: The nose must be gently irrigated with a small volume of warm, sterile saline solution • Sun therapy or “sun bath”: it is done while in kangaroo position twice a day through the window • The child must wear only his diaper, which is folded or left short. • The child’s eyes are shielded by the caregiver’s hand. • Massage : it is done daily, in strict kangaroo position • Visits: precautions t must be observed and explained to the family. • Only few people could visit the infant at one time • Visitors must wash carefully their hand before approaching him. • The baby must not be manipulated by visitors. • People with respiratory infection, must use a mask • Appropriate clothing: The ‘kangaroo’ child’s clothes must leave a greater area of skin uncovered to remain in contact with the caregiver’s skin Infant’s clothes must be made from cotton and wash with a non alcalin soap The baby must be free of any straps, bracelets, amulets, necklaces, rings or earrings on or around any part of his body.
Teaching alarm/danger signs • Parents must be trained to be able to recognize the alarm/danger signs for which the family must seek care immediately • Blood in the stool • Difficult breathing (fast breathing, grunting, repeated apneas), • Lethargy, moving and eating less than usually. • Refusing to feed. • Vomiting everything ( 2 or more episodes of continuous vomiting) • Uninterrupted crying ( more than 3 hours) • The nurse has to assess the parent’s knowledge, reinforcing and correcting any misunderstanding++ • Parents must be aware of signs such as ‘pushing ’before a bowel movement, hiccups and sneezing which are normal for children
Management of the oxygen equipment • When children are discharged home with oxygen families must know well the equipment (neonatal cannula, humidifier, cylinder, flow meter, among others), as well as the correct way to use and manipulate it • The nurse has to demonstrate to parents how to use oxygen and to assess the parent’s knowledge, reinforcing and correcting any misunderstanding they could have • Parents need to receive information for easy access to oxygen • Some precautions should be respected • Prevent the water from the humidifier from going into the cannula • Wash the oxygen humidifier with soap and water every other day • Change the water in the humidifier daily. • Make sure that the water bubbles which prove that oxygen is flowing. • Check the gauge to know how much oxygen is still available • Keep oxygen far from candles, matches or open flames
Adaptation to the KMC Nutrition • The kangaroo adaptation to the nutrition of a preterm infant is “a process of social and physical adjustment for the mother and family to the Kangaroo Mother Care Method” • It is done through an education process with social and emotional support • It is vital for the success of the kangaroo nutrition • Is done after the kangaroo position adaptation • Existing open door policy for parent to stay with their child • The mother should be recognized as the baby’s primary care provider • her stay next to her child should be done comfortable • The health team is a central person to advocate and promote satisfactory breastfeeding • The support given during the breastfeeding period should: • Develop the mother’s confidence ,paying attention to the mother’s problems, • Provide precise and practical information about the child’s needs • Offer options and allow the mother to make decisions • Give timely pertinent information on technical and scientific content
Adaptation to KMC nutrition • Reassure the mother that she is able to feed her baby • Train the mother to watch the baby completes at least 6 suctions, alternated with pauses to breathe • The weight test can be used to determine the volume of ingested breast milk, but it may stress the mother, daily weight is enough • Breastfeeding preterm infants is difficult and demanding • Actively counsel her to: • Feed the baby every 1½ -2 hours • Wake the baby up for feeding • Keep the baby at the breast longer • Let the baby takes long pauses and breastfeed more slowly • Do not interrupt breastfeeding if the baby is still trying to suckle • Express some milk before the baby attaches if milk flow needs to be reinforced • Breastfeed the baby with hind milk if the baby does not gain weight WHO, 2003
Feeding preterm infants • Feeding based on maternal milk from his own mother plus vitamins A,D,E and K: • Exclusive, with no fortifiers or supplements • Fortified (fortifiers added to extracted milk) • Supplemented with artificial milk for preterm infants • Supplemented with fortified and pasteurized human milk from a donor (preterm or full term) • Feeding based on artificial formula for preterm infants • Exclusive or supplementary use of other forms or oral or enteral nutrition; protein hydrolysats, element and semi-element preparations • Preterm babies do not demand to be fed until they reach full term nursing must be done on a schedule rather than on demand
Alternative Feeding Methods 1.Cup/spoon/syringe/dropper • Does not interfere with breastfeeding • Cup is easy to wash • Safe • Small baby gets the quantity she/he needs • Cup-feeding can complement breastfeeding if the baby is weak or tired WHO , 2006
Alternative feeding techniques Cup-Feeding Technique • Measure the quantity of milk needed into a cup • Hold the baby in semi-upright position • Touch the baby’s lips with the cup • Do not pour the milk into the baby’s mouth • Allow the baby to lap or sip the milk and swallow at own rate • The baby stops feeding when his/her mouth closes and doesn’t show further interest in feeding WHO EURO, 2002 BMJ, 2004
Evaluation of the mother adaptation to KMC • The evaluation of the quality of the in-hospital kangaroo adaptation of the mother is done taken into consideration: • The mother’s readiness to take the child home or to a mother-child kangaroo rooming-in • The mother capacity to nurse the child • the child’s tolerance to the kangaroo position • A scale is used to assess 11 points of mother/family readiness • Ability to place the child to the breast and good breastfeeding technique • Ability to manipulate the child to awaken him, feed him and change him • Stimulation and response to the child’s signals • Security and confidence in caring for the child • Appropriate milk production • Knowledge about the methodology of the KMC • Acceptance and application of the KMC • Familial and socio emotional support • Length of in-hospital adaptation • Mother’s health status and the possibility to attend daily follow up
Decision of Discharge Use of the Kangaroo adaptation Scales • The decision to discharge the infant is taken by common agreement between parents and the health team • The decision to discharge the infant in taken only is all aspects of adaptation are finalized, a format is used to standardize this assessment • If some aspects of adaptation are not finalized the child must stay: • In minimal care unit, or • In Kangaroo rooming-in accommodation++ with his mother until the adaptation is complete
Discharge after in hospital KMC adaptation (1) A child is ELIGIBLE for discharge whether to rooming-in accommodation, or home, regardless of his weight or gestational age if : • The child’s in-hospital kangaroo adaptation has been successful • He is regulating his temperature in KP • He has an adequate sucking –swallowing -breathing coordination • The child has had adequate weight gain in KP for at least 2 days • The child completed his treatment if any • If the child is receiving oxygen through a cannula, it must be below ½ l/min. • There is a KMC Program available able to offer adequate follow up
Discharge after in hospital KMC adaptation (2) A mother is ELIGIBLE to have her infant discharged if : • She was trained in the KMC method with a successful adaptation • She feels able to care for her child using KMC at home • She has adequate breastfeeding and milk extraction techniques • She is physically and mentally able to care for her child A family is ELIGIBLE to have her infant discharged if the family : • Has the will to be trained in KMC and understand the method • Is available and feels able to care for the baby at home • Will comply with follow up, medical appointments, breastfeeding schedule and drugs prescription , adapt to the changes due to KMCand support the mother
KMC in rooming- in accommodation • In many countries, preterm or LBW infants are not directly discharged home from the delivery/recovery room or neonatal units • Usually the mother remains with her infant, in the KMC ward until the end of the initial observation period: daily follow up until the child gains 15 g/kg/day • Some factors influence the decision to discharge to KMC ward • Economic factors, family not able to pay for daily transportation • Rural or "difficult to reach” area with ambulatory KMC • in case of limited confidence in the mother’s ability to care to her infant The main benefits of rooming-in hospitalization in kangaroo position compared to hospitalization in minimal neonatal care unit are: • A better compliance with KP and breastfeeding supported by the staff • A shorter mother - child separation, supporting a better bonding • A reduction of nosocomial infection as the mother is caring for her baby Discharge criteria for rooming-in are ruled by week
Organizationof KMC rooming-in Infrastructure: • It may be just a room, for one mother or a collective room for few mothers • A bathroom must be available for the mothers’ personal hygiene • If possible, an additional room should be available with tables and chairs, in order for several mothers and / or families to gather and have training or recreational sessions and / or talks Material resources: • Beds, waste baskets, Kangaroo Mother Program forms (clinical records, identification cards, leaflets), milk extraction pumps, a refrigerator for milk storage, materials for milk collection (sterile jars, syringes, gloves) and models or teaching resources Human resources: • a pediatrician /MD for the daily checkup of infants and an obstetrician /gynecologist to care for mothers • A nurse responsible for teaching and for the supervision of KMC • An auxiliary nurse full time, to support the kangaroo position and nutrition • Social worker and psychologist should be available if socio-emotional risk factors are identified
Cultural adaptation to KMC rooming-in • In some countries (India, Pakistan, Bangladesh) the mother-in-law is the one deciding what will be the tasks assigned to the new mother when she will return home, the implementation of KMC requires her involvement • Kangaroo adaptation and rooming-in should be implemented in a place where the mother-in-law can come and be an active participant; therefore she will understand from experience the importance of KMC allowing the new mother to hold her baby in kangaroo position 24 hours a day, upon returning home, and following the recommendations of the Kangaroo Mother Care Program. • Rooming-in may be an opportunity for hospitals to provide adequate nutrition to nursing mothers as well as given information on nutrition, immunization and other interesting topics for the mothers
Conclusion • Adaptation to Kangaroo position and kangaroo nutrition should be imitated as soon as possible in hospital • It a challenging task for the health team • Successful in- hospital adaptation to KMC is the key for a safe early discharge and successful ambulatory implementation of the KMC program