Download
1 / 36
360 likes | 371 Views
This study analyzes the characteristics, performance measures, and in-hospital outcomes of the first one million stroke and transient ischemic attack (TIA) admissions in the Get With The Guidelines-Stroke program from 2003 to 2009.

E N D
Characteristics, Performance Measures, and In-Hospital Outcomes of the First One Million Stroke and Transient Ischemic Attack Admissions in Get With The Guidelines-Stroke Gregg C. Fonarow, MD; Mathew J. Reeves, PhD; Eric E. Smith, MD, MPH; Jeffrey L. Saver MD; Xin Zhao, MS; DaWai Olson, PhD, RN; Adrian Hernandez, MD, MHS; Eric D. Peterson, MD, MPH; Lee H. Schwamm, MD on behalf of the Get With The Guidelines Steering Committee and Hospitals Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Disclosures GWTG-Stroke is sponsored by the AHA/ASA and is also supported in part by an unrestricted educational grant from Merck/Schering-Plough Pharmaceutical. The individual author disclosure are listed in the manuscript Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Background • Stroke results in substantial morbidity and mortality. • While evidence-based guidelines for stroke and TIA care have been developed along with improved diagnostic and treatment modalities, there are gaps, variations, and disparities in how these are applied. • Furthermore many hospitals may not have the systems, organization, staff, and equipment to effectively diagnose, manage, and treat acute stroke patients. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Background • The Get With The Guidelines (GWTG)-Stroke Program was developed by the AHA/ASA as a national stroke registry and performance improvement program with the primary goal of improving the quality of care and outcomes for stroke and TIA as well as serve as a scientific resource for new information. • Although several prior studies have described the quality of care and outcomes for patients hospitalized with stroke and TIA, uncertainty remains about care quality and clinical outcomes for contemporary populations of patients hospitalized with stroke and TIA. • Furthermore, little is known regarding temporal trends and whether there have been improvement in clinical outcomes among hospitals participating in GWTG-Stroke. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Objectives • The objectives of this study were to analyze the characteristics, performance measures, in-hospital outcomes, and temporal trends in the first 1,000,000 acute ischemic stroke, intracerebral hemorrhage, subarachnoid hemorrhage, and TIA admissions from 1,392 hospitals that participated in the GWTG-Stroke Program from 2003 to 2009. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Methods • GWTG Stroke is an ongoing, voluntary, observational registry and a continuous performance improvement program for patients hospitalized with stroke or TIA. • A web-based Patient Management Tool provides decision support at the point-of-care, on-demand reporting and patient education features (Outcome, Cambridge, MA). • Patient data were abstracted by trained hospital personnel. These included demographics, medical history, initial CT findings, in-hospital treatment and events, discharge treatments, treatment contraindications, counseling, in-hospital mortality, and discharge destination. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Methods • Trained hospital personnel ascertained consecutive patients admitted with acute ischemic stroke by either prospective clinical identification, retrospective identification using ICD-9 discharge codes, or a combination. • Methods used for prospective identification varied, but included regular surveillance of ED records, ward census logs, and/or neurological consultations. • The eligibility of each acute stroke or TIA admission was confirmed at chart review prior to abstraction. • Performance and quality measures were collected and reported. • Outcomes included: % of pts with a short length of stay (LOS <4 days); % discharged home, and in-hospital mortality. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Statistical Methods • Characteristics, performance measures, in-hospital outcomes, and temporal trends were evaluated. P-values were based on chi-square rank based group means score statistics for all categorical row variables (equivalent to Wilcoxon test for two levels). • GEE multivariable logistic regression models were developed to quantify how performance measures, in-hospital mortality, discharge home, and LOS changed on a continuous basis by quarter from 2003 to 2009 and reported as cumulative change over 6 years adjusting for patient and hospital variables. • Since the makeup of participating hospitals may have changed over time in GWTG-Stroke, we also performed a separate set of analyses for temporal trends among core hospitals which were participating by 2004 and contributed cases in all subsequent quarters of the study. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Results • From April 1st 2003 to August 24th 2009, there were 1,000,000 patients with stroke or TIA entered from 1392 GWTG-Stroke participating hospitals. • There were 601,599 (60.2%) ischemic strokes, 108,671 (10.9%) intracerebral hemorrhage s, 34,945 (3.5%) subarachnoid hemorrhages, 26,977 (2.7%) strokes not classified, and 227,788 (22.8%) TIAs. • Stroke and TIA patients enrolled by year • 2003 N= 18,971 (starting April 1st 2003) • 2004 N= 41,065 • 2005 N= 96,139 • 2006 N= 167,666 • 2007 N= 220,734 • 2008 N= 262,785 • 2009 N= 159,083 (through August 24th, 2009) Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Enrollment in GWTG-Stroke by Quarter Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Hospital Participation in GWTG-Stroke by State N=1392 Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Hospital Characteristics 1392 GWTG-Stroke Participating Hospitals Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Hospital Participation in GWTG-Stroke • Hospitals in every state participate in the GWTG-Stroke Program. • Of participating hospitals, 39.5% were non-academic institutions. • Divided by regions, the South has the largest number of participating hospitals (n=500), followed by the Northeast (n=346), the Midwest (n=325), and the West (n=252). • GWTG-Stroke participating hospitals account for an estimated 32.3% of US acute care hospitals. • In 2008, there were 156,000 ischemic stroke patients entered into GWTG-Stroke out of 663,000 expected in the US (25%) and 47,937 hemorrhagic stroke patients entered out of 117,000 expected in the US (41%). Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
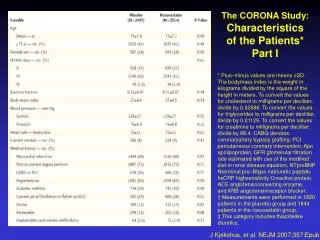
Patient Characteristics Total Cohort Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Patient Characteristics by Event Type Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Patient Characteristics by Event Type Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Patient Characteristics in GWTG-Stroke • For the 1,000,000 acute stroke (n=772,212) and TIA (n=227,788) admissions entered into the program, the mean age was 70.1 ± 14.9 years and over half (53.5%) were women. • IS and TIA patients were older, more likely to be men, less likely to be smokers, and more likely to have medical co-morbidities than ICH and SAH patients. • ICH patients had a relatively high prevalence of vascular risk factors, but not as high as for IS or TIA patients. • Patients with stroke not classified were most similar to IS patients. • SAH patients were more likely than IS or TIA patients to be younger, female, non-white and to be cared for in larger academic hospitals. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Performance Measures by Event Type Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Quality Measures by Event Type †Data collected starting 2008 Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Acute Stroke and TIA Care 2003-2009 Temporal trend P value is <0.0001 for each measure Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Acute Stroke and TIA Care 2003-2009 Summary Performance Measures Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Acute Stroke and TIA Care 2003-2009 All-or-None Performance Measure *Adjusted for age, gender, race, medical history of Afib, stroke/TIA, CAD/prior MI, carotid stenosis, diabetes, PVD, hypertension, dyslipidemia, smoking, arrival mode (EMS vs. other), on/off hour presentation (7 am-6 pm MF vs other), hospital characteristics of region, number of beds, annual stroke volume, academic vs. not. Overall cohort also adjusted for stroke type (IS, SNC, SAH, ICH, TIA). Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Performance Measures in GWTG-Stroke • In each successive year there were clinically meaningful and statistically significant improvements in all 7 individual PM. • The absolute improvement from 2003 to 2009 ranged from +4.3% for discharge antithrombotics to +51.0% for smoking cessation (P <.0001 for all comparisons). • IV tPA use in eligible patients increased from 29.7% to 71.6% (+41.9%), P<0.0001. • There was substantial and significant improvement in the all-or-none care measure from 2003 to 2009, 44.0% to 84.3% (+40.3%), P<0.0001 overall and for each cerebrovascular event type. • There was also an increase in composite care from 72.3% to 93.1% (+20.8%), P<0.0001 overall and for each event type. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Stroke-Related In-Hospital Outcomes by Cerebrovascular Event Type Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Clinical Outcomes by Cerebrovascular Event Type + Adjusted for patient and hospital characteristics. See manuscript for variables Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Clinical Outcomes in GWTG-Stroke • SAH and ICH patients had substantially higher in-hospital mortality rates, were less likely to be discharged home, and were more likely to be discharged to a SNF or hospice compared to IS patients. • As expected, in-hospital mortality was very low in patients hospitalized with TIA (0.3%). • Adjustment for potential confounding variables and clustering of data within hospitals did little to attenuate the cerebrovascular event type related differences for clinical outcomes. • The adjusted OR for in-hospital mortality for ICH compared to IS was 5.8; for SAH it was 5.4. • After adjustment the odds of being hospitalized longer than 4 days remained significantly elevated for SAH and ICH compared to IS. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Mortality 2003-2009 Temporal trend P value for ischemic stroke (P<0.0001), intracerebral hemorrhage (P=0.0036), subarachnoid hemorrhage (P=0.0106), transient ischemic attack (P=0.2091). Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Clinical Outcomes 2003-2009 Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Clinical Outcomes 2003-2009 * Adjusted for patient and hospital characteristics. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Clinical Outcomes by Calendar Year for Ischemic Stroke Patients Total Ischemic Stroke Patients N = 601,599 Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Outcomes for Ischemic Stroke Odd Ratios for 6 Year Change 2003 to 2009 +Adjusted for PATIENT CHARACTERISTICS of age, gender, race, medical history of atrial fibrillation, previous stroke/TIA, coronary artery disease, carotid stenosis, diabetes, peripheral vascular disease, hypertension, dyslipidemia, smoking, arrival mode (EMS vs. other), on/off hour presentation (7 am-6 pm M-F vs. other), and HOSPITAL CHARACTERISTICS of region, number of beds, annual stroke volume, and teaching hospital vs. not. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Temporal Trends in Clinical Outcomes • There were temporal trends for improvement in clinical outcomes from 2003 to 2009. • The portion of patients discharged home in 2003 was 53.8% compared to 57.1% in 2009 (P<0.0001) and LOS > 4 days was seen in 40.1% in 2003 compared to 35.6% in 2009. • After adjustment, the portion of patients with hospital LOS >4 days declined significantly, adjusted OR 0.72, 95% CI 0.69-0.77, P<0.0001. • In-hospital mortality also declined significantly over time, unadjusted OR 0.87, 95% CI 0.80-92, P<0.001, 2003 to 2009, but after risk adjustment was only significant for ischemic stroke and TIA. • There was a 10% risk adjusted reduced odds of mortality in patients with IS from 2003 to 2009. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Limitations • Data were collected by medical chart review and are dependent upon the accuracy of documentation and abstraction. • Residual measured and unmeasured confounding variables may have influenced the findings. • Further study will be needed to determine if these improvements in outcomes are due to improved care (faster in-hospital response times, guideline-adherence, and reduced complications or errors), secular trends, or other reasons. • These findings may not apply to hospitals that differ in patient characteristics or care patterns from GWTG-Stroke Hospitals. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Conclusions • GWTG-Stroke is the largest registry and performance improvement programs for hospitalized stroke and TIA patients, with data from 1,000,000 admissions including more than 600,000 IS, 100,000 ICH, 30,000 SAH, and 225,000 TIA admissions. • This study has characterized the demographics, performance measures, and in-hospital clinical outcomes in a very broad cohort of acute stroke and TIA hospitalizations from every state in the country. • Among GWTG-Stroke participating hospitals there were substantial improvements over time in performance measures, overall and for each cerebrovascular event type. • Composite care performance increased substantially from 72.3% to 93.1% (+20.8%) from 2003 to 2009. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Conclusions • Among hospitals participating in GWTG-Stroke, there have been reductions in LOS and mortality at discharge over the past 6 years in the patients with acute ischemic stroke. • These findings persist after adjustment for patient and hospital characteristics. • Further research is warranted to determine if these reductions in mortality are due to increased adherence to inpatient care process measures, secular trends, unmeasured confounders, or other reasons. • Other factors might include increased public education and awareness, increased use of EMS, improvements in in-hospital response times, guideline-adherence, and prevention of complications or medical errors. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22
Conclusions • This study demonstrates the ongoing value of GWTG-Stroke as an integrated stroke and TIA national registry providing national surveillance, supporting vigorous efforts to improve evidence-based stroke/TIA care, and fostering innovative research. Fonarow GC et al. Circ Cardiovasc Qual Outcomes. 2010 epub Feb 22