Download
1 / 67
670 likes | 696 Views
Learn about different classes of antidysrhythmic drugs, their actions on the heart, side effects, and nursing interventions. Explore specific medications like Quinidine, Procainamide, and Lidocaine.

E N D
Antidysrhythmic and Antihypertensive Agents NURS 1950 Pharmacology Nancy Pares, RN, MSN
Objective 1: Define the term ‘ectopic site’. • Heart beat arises outside the sinoatrial (SA) node
Objective 2: Define the terms • Arrhythmia or dysrhythmia • Variation of normal rhythm-usually associated with cardiac • An electrical activity initiated by a spontaneous discharge
Objective 3: Describe the actions of the antiarrhythmic drugs • Decrease the automaticity of the cardiac tissues distant from the sinoatrial node. • Alter the rate of conduction • Alter the refractory period between consecutive contractions.
Actions: Antiarrhythmic agents • Classed according to action • Class I: myocardial depressents-inhibit sodium ion movement causing depolorization • Ia: prolongs electrical stimulation (in cell) prolongs refractory time between impulses Ib: shortens the duration of the e-stimulation and the time between impulses Ic: most potent-slows conduction rate through atria and ventricles
Antirrhythmics: Actions Class II: beta-andrenergic blocking agents -block sympathetic stimulation Class III: slows the rate of electrical conduction and prolongs refractory time -potassium channel blocking
Antirrhythmic class actions Class IV:blocks calcium ion flow-prolongs elec stimulation and slows AV node conduction Misc: Adenosine and Digoxin: not related to any other agents
Objective 4: Identify actions, results and uses of major antirrhythmics • Objective 5: List the side effects of antirrhythmics
Class Ia: Sodium channel blockers • Includes: • Disopramide phosphate (Norpace) • Procainamide HCL (Pronestyl) • Quinidine gluconate (Duraquin) • Quinidine polygluconate (Cardioquin) • Prototype: Procainamide (Pronestyl)
Quinidine (Quinidex, Duratab) • -derived from the cinchona bark • -cardiac depressant effects: reduces excitability of the cardiac muscle, prolongs refractory period between consecutive contractions • Allows the sinoatrial node to take over
Quinidine • Used for atrial tachycardia, flutter and fibrillation. • Side effects severe: 1/3 of clients must d/c use
Quinidine • S/E: • GI distress • CV disorders • Rashes, respiratory arrest, hemolytic anemia, agranulocytosis • Hypersensitivity • Cinchonism: tinnitus, nausea, HA, dizziness impaired vision, vertigo
Quinidine • Nursing Implications: • Can reduce problems if nurse: • Avoid use in CHF patients • Monitor digitalis levels (if on digitalis) • Monitor potossium (K+) levels • Monitor sodium (Na+) levels
Quinidine • Routes: • Oral with meals • Parenteral: give slowly
Procainamide (Pronestyl, Procan SR) (Ia) • Uses:ventricular arrhythmias (best), atrial fibrillation(helpful), paroxysmal atrial tachycardia (PAT) • S/E: GI distress, ventricular tachy, hypotension and hypersensitivity • Allergy most likely if allergic to ‘caine’ drugs (related to local anesthetics) • Can cause agranulocytosis: lupus like syndrome
Disopyramide (Norpace, Rythmodan) • S/E: hypotension, tachyarrythmias, anticholinergic effects • Has lower incidence of adverse effects than quinidine or procainamide • Oral dosing
Class Ib: Sodium (Na+)Channel Blockers • Lidocaine (Xylocaine) • Mexiletine (Mexitil) • Phenytoin (Dilantin) • Tocainide (Tonocard)
Lidocaine (Xylocaine, Xylocard) • Use:Preventricular contractions (PVC), cardiac glycoside-induced tachyarrhythmias, cardioversion • Action: very rapid onset (IV), short acting
Lidocaine (Xylocaine, Xylocard) • S/E/Route: • Excessive decrease in cardiac electrical conductivity • Hypotension, bradycardia, dizziness; CNS effects • Hypermetabolism (malignant hyperthermia • ineffective if given orally (metabolized in liver)
Lidocaine (Xylocaine, Xylocard) • Nursing Interventions: • Continuous EKG • Look at bottle before giving-should not contain preservatives or epinephrine
Phenytoin (Dilantin) (Ib) -standard classification is neuroleptic, but used for arrythmias caused by cardiac glycoside intoxication Action: decreases automaticity of cardiac muscle, increases rate of conduction of the cardiac electrical impulses
Phenytoin (Dilantin) • S/E/ Route: • Neurological disturbances: peripheral neuropathy, diplopia, ataxia, vertigo, drowsiness, confusion • GI disturbances • Skin rash
Tocainide (Tonocard)(Ib) • Similar to lidocaine • Nursing Interventions: • Given orally only • Monitor EKG • Client teaching: s/e and when to call MD • S/E: • Dizziness, nausea, parethesia, numbness, restlessness, tremor, GI distress, blood dyscrasias • Should not be used in 2nd or 3rd degree AV block without a pacemaker
Mexiletine HCL (Mexitil) • Action: similar to lidocaine • Use: ventricular arrhythmias • S/E/route: • N/V, heartburn, dizziness, tremor, impaired coordination • Given orally
Class IC: Sodium(Na+) Channel blockers • Flecainide (Tambocor) • Encainide (Enkaid) • Rythmol
Flecainide acetate (Tambocor)Encainide HCL (Enkaid) • Action: local anesthetic • Use: ventricular arrhythmias • S/E/route: • Can cause new or worsen arrhythmias • High degree of negative inotropy • Dizziness, visual disturbances, HA, nausea, fatigue, chest pain
Propafenone HCL (Rythmol) • Local anesthetic, membrane stabalizing, some beta blocking effect • Use: life threatening ventricular arrhythmias • S/E: may cause new or worsen existing arrhythmias, dizziness, GI disturbances, may see 1st degree AV block • Nursing Interventions: monitor with EKG • Contraindications: uncontrolled CHF, brady, bronchospasm, severe hypotension
Class II: Beta adrenergic blocking agents • Acebutolol (Sectral) • Esmolol (Brevibloc) • Propranolol (Inderal) • Action: • Inhibits cardiac response to sympathetic nerve stimulation by blocking the beta receptors; reduces heart rate, systolic BP and cardiac output.
Class II: Beta adrenergic blocking agents • Use: • Ventricular arrhythmias • Sinus tachycardia • Paroxysmal atrial tachycardia (PAT) • Premature ventricular contractions (PVC) • Tachycardia associated with atrial flutter,or fibrillation
Class II: Beta adrenergic blocking agents • S/E: • What would we expect to see? • Slow HR, orthostatic hypotension, SOB, painful urination, wt gain > 2 lbs/day, insomnia, drowsiness, confusion • Mask the signs of hypoglycemia • Nursing Interventions: • Take pulse and report below 50, rise slowly, report symptoms, diabetics monitor BS closely
Class III: Potassium(K+)channel blockers • Amiodarone (Cordarone) • Dofetilidide (Tikosyn) • Sotalol (Betaspace)
Amiodarone hydrochloride (Cordarone) • Action: • Prolongs the action potential of the atrial and ventricular tissues • Antagonizes (non competitive) the alpha and beta receptors causing vasodilation • Use: • Life threatening arrythmias non responsive to other agents
Amiodarone hydrochloride (Cordarone) • S/E/Route: • Fatigue, tremors, sleep disturbances, numbness, ataxia, confusion, exertional dyspnea, non-productive cough, pleuritic chest pain, photosensitivity • s/e often cause clients to d/c use • > 400mg/day cause problems • Given oral or IV
Amiodarone hydrochloride (Cordarone) • Nursing interventions: • Loading dose is needed • Watch monitor for new arrhythmias • Dose adjustment is difficult • Monitor/teach about post treatment arrhythmias • Wear sunscreen
Class IV: Calcium (Ca+) channel blockers: Diltiazem (Cardizem) • Action/Use: • slows conduction through the AV node causing relaxation of the coronary and peripheral vessels • Dysrhythmias • S/E: • HA, dizziness, lower extremity edema, increases digoxin and quinidine levels
Diltiazem (Cardizem) • Nursing interventions: • Do not crush or chew extended release tablets • Use with caution with other CV agents: digoxin, beta adrenergic blockers • Monitor for partial or complete heart block, heart failure
Miscellaneous antidysrhythmics • Adenosine (Adenocard) • Digoxin (Lanoxin) • Ibutilide ( Corvert)
Adenosine (Adenocard) • Action/Use: • Strong depressant effect on SA and AV nodes-slowing conduction • Treatment of paroxysmal supraventricular tachycardia (PST) • Physiologic roles: energy transfer, prostoglandin release, inhibits platelet aggregation, coronary vasodilation, suppresses heart rate
Adenosine (Adenocard) • S/E • Flushing, SOB, chest pressure, nausea, HA, dizziness, peripheral edema, anxiety • Half life is 10 seconds—s/e are not lasting
Objective 6: Describe nursing implications associated with antiarrhythmics • Give meds on scheduled time • Assess 6 cardinal signs of CV disease • Chest pain, dyspnea, edema, fatigue, syncope, palpitations (C-D-E-F-S-P) • Lab tests: CV markers (enzymes) • Physical assessment of client: include EKG readings
Objective 6: Describe nursing implications associated with antiarrhythmics • Be prepared for emergency care • O2 as needed • Assist with ADLs • Client education • Lifestyle • Medications • Report s/e and adverse effects
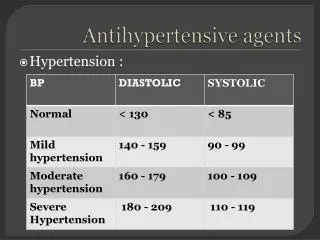
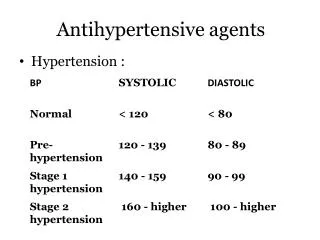
Objective 7: define essential hypertension • Also called ‘idiopathic’ • ‘essentially’ no known cause
Objective 8: List the factors which determine Blood Pressure • Cardiac output • Increase cardiac output=increased BP • Peripheral vascular resistance (PVR) • Lumen inside vessels will constrict and dilate which determines PVR • Total Blood volume • (see diagram in Adams)
Objective 9: Identify diuretics used as antihypertensives • Carbonic anhydrase inhibitors • Rarely used for hypertension • Thiazides • Loop diuretics • Potassium sparing • Used in combination therapy with thiazide or loop diuretic
Diuretics: common actions/use • Deplete blood volume • Help excrete sodium • Dilate peripheral aterioles • Specific action unknown • Often used in combination • Potentiates activity of other antihypertensives • Cheap and effective
Diuretics • Thiazides: • Most effective if creatinine clearance >30 • Most commonly used: Hydrochlorothiazide • Loop diuretics • Used when creatinine clearance <30 • Most commonly used Furosemide (Lasix)
Diuretics • Potassium sparing • Contraindicated with renal disease, pregnancy, gout or kidney stones • Nursing interventions: • Monitor labs (WBC decrease, liver and kidney) • Client education • Most commonly used: Spirolactone (aldactone) • S/E: gynecomastia, testicular atrophy, hirsutism
Objective 10: Identify non-diuretic antihypertensives Beta-adrenergic blockers Angiotensin converting enzyme (ACE) inhibitors Calcium channel blockers