Download
1 / 12
120 likes | 534 Views
Correlating EMG exercise tests with genotype International Conference on the Nondystrophic Myotonias. Marianne Arzel-Hézode, Emmanuel Fournier Centre de référence des Canalopathies Musculaires Hôpital La Salpêtrière, Paris, France.

E N D
Correlating EMG exercise tests with genotypeInternational Conference on the Nondystrophic Myotonias Marianne Arzel-Hézode, Emmanuel Fournier Centre de référence des Canalopathies Musculaires Hôpital La Salpêtrière, Paris, France
Muscle channelopathiesPatients with EMG and genetic diagnose : N=171(La Salpêtrière, 1996-2007) • Myotonic syndromes N = 104 • Myotonia CLCN1 (A313T, P480L…) 33 • Paramyotonia SCN4A (T1313M, R1448C/H/G, Q270K…) 40 • SCM («PAM ») SCN4A (G1306A/V, V445M, A715T, S804N…) 31 • Periodic paralysis N = 67 • HyperPP SCN4A (T704M, R675G, I693T…) 25 • HypoPP-1 CACNLA1 (R528H, R1239H) 24 • HypoPP-2 SCN4A (R672G/H, R1135H…) 6 • Andersen (ATS) KCNJ2 (C54F, T75M, C154F/Y, T309I…) 12
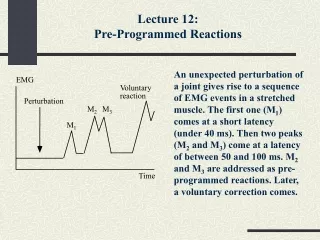
Supramaximal Nerve stimulation MU2 MU1 CMAP Electrophysiological abnormalities triggered by pioneer tests • CMAP amplitude decreases were observed : • during 10 Hz repetitive nerve stimulation in myotonic syndromes • Lambert et al. 1952, Bastron 1960, Ricker et al. 1973, Brown 1974, Aminoff et al. 1977 • after a single short exercise test in myotonic syndromes • Streib et al. 1982, Streib 1987 • after a long exercise test in periodic paralyses • Mc Manis et al. 1986, Kuntzer et al. 2000 • Interpretation • CMAP amplitude correlates with the number of functional muscle fibers • Its decrease is an index of muscle weakness experienced after exercise • Exercise tests = provocative tests
I Long exercise test Right hand (ulnar - ADM) Exercise lasting 5 minutes (respecting regular brief rests) Recording every 5 minutes during 40-45 minutes post-exercise rest II Repeated short exercise test Left hand (ulnar - ADM) 3 exercises of 10 seconds with 1 minute between each trial Recording every 10 seconds for 50 seconds after each exercise 1st EMG protocol (1996, revised 2000) Ann Neurol 2004 • PatientsN = 51 • Chlore Myotonia (MC) 6 • Paramyotonia (PC) 16 • Sodium Myotonia (SCM) 8 • Sodium HyperPP 6 • Sodium HypoPP-2 2 • Calcium HypoPP-1 13 • Control Subjects N = 41 • III • Search for myotonic discharges with needle EMG • Deltoid, extensor digitorum communis, 1st interosseus dorsalis, tibialis anterior
Repeated short exercise test Chloride Myotonia - 61 % - 45 % - 20 % « Warm-up » phenomenon Type II Post-exercise myotonic potentials (PEMP) Sodium Paramyotonia - 48 % - 64 % • Aggravation with exercise repetition • Stiffness-weakness continuum Type I
Five main EMG patterns Fournier et al.Ann Neurol 2004
I Repeated short exercise test Right hand (ulnar -ADM) 3 exercises of 10 s with 50 s rest intervals II Cooling test Left hand (ulnar -ADM) Ice bag for 7 minutes Repeated short exercise test at cold 3 exercises of 10 s with 50 s rest intervals 2nd EMG protocol for distinguishing myotonic syndromes (2003) Ann Neurol 2006 • PatientsN = 61 • Chlore Myotonia 18 • Paramyotonia (PC) 22 • Sodium Myotonia (SCM) 14 • DM1/DM2 7 • Control Subjects N = 31 • III • Search for myotonic discharges • Needle EMG of deltoid, EDC, 1st IOD, tibialis anterior Total exam lasts 20 minutes
Worsening of the abnormalities observed at room temperature Pattern changes Improvement of EMG distinctions with cold - 82 % - 90 % - 93 %
80 % SCN4A 100 % SCN4A EMG guides toward myotonic syndrome genotypes 86 % 85 % 60 % 14 % 15 % 20 % 20 % Ann Neurol 2006
EMG Protocols’ Objectives • Diagnosis • Disclose functional abnormalities by mimicking provocative circumstances • Explain symptoms (electrical response changes as index ) • Determine differential diagnosis of weakness episodes • And more : distinguish closer clinical phenotypes • Guide molecular diagnosis • Isolate physiopathological mechanisms • Look for therapeutical advances