Download
1 / 20
220 likes | 495 Views
Laparoscopy for Splenic Conditions. George W. Holcomb, III, M.D., MBA Children’s Mercy Hospital Kansas City, MO. Splenic Conditions. ITP Spherocytosis Splenic cysts Wandering spleen. J Pediatr Surg 28:689-692, 1993. Pre-Operative Preparation. Ultrasound

E N D
Laparoscopy for Splenic Conditions George W. Holcomb, III, M.D., MBA Children’s Mercy Hospital Kansas City, MO
Splenic Conditions • ITP • Spherocytosis • Splenic cysts • Wandering spleen J Pediatr Surg 28:689-692, 1993
Pre-Operative Preparation • Ultrasound • Often done by pediatrician, hematologist • Rarely needed for splenectomy, except may be useful for extremely large spleen • CT Scan – Useful in planning splenic cystectomy • WinRho • Bone marrow stimulant • Usually used to platelet count • Useful pre-operatively to platelet count in ITP pt. • Immunizations –Pneumococcus (Prevnar, Pneumovax)
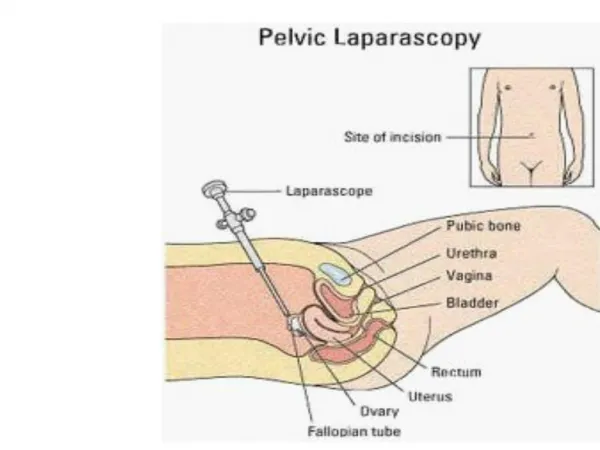
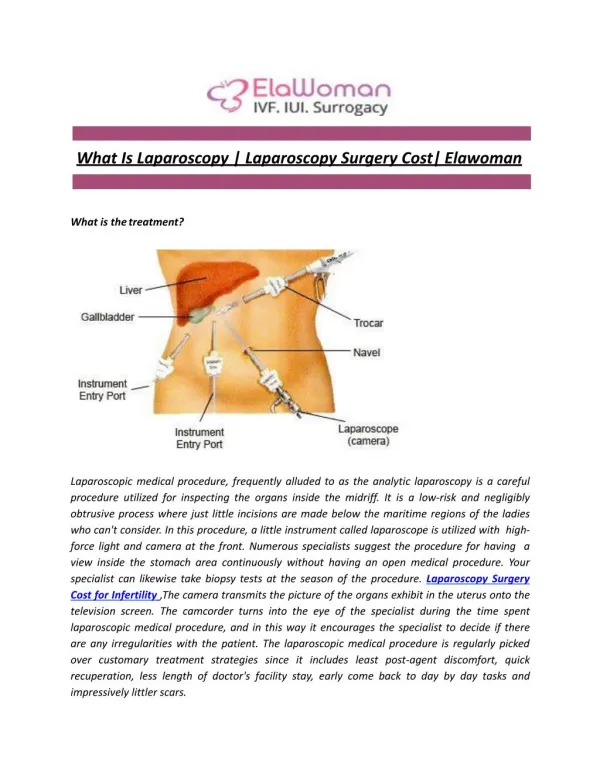
Laparoscopic Splenectomy • ITP, spherocytosis • Port placement • (2) cannulas (5, 12) • (2) stab (3 mm) incisions • Instruments • Harmonic scalpel (5 mm) • Articulating stapler (12 mm)
Laparoscopic Splenectomy Operative Steps • Divide spleno-colic ligament, then short gastrics • Clip artery • Autotransfuse pt • Protects stapler malfxn
Laparoscopic Splenectomy Operative Steps • Divide spleno-renal lig. • Articulating stapler across hilum • Bag specimen, morcellate extracorporally
Issues • How large is too large? • Measurement (LeClair) • Earlier splenic artery ligation helpful • Can divide spleen (spherocytosis) with harmonic, if necessary
Issues • Postoperative platelet ct. > 500,000 • Reports of splenic vein/portal vein thrombosis following splenectomy (open and laparoscopic) • Baby aspirin ( 81 mg) QD for 6 mos • Re-check at 3 months & 6 months
Splenic Cysts • Primary • epithelial lining • Pseudocysts (secondary) • no epithelial lining • often develop after trauma
Splenic Cystectomy • First step is decompression of cyst
Splenic Cystectomy • Excise cyst as close as possible to splenic parenchyma with harmonic scalpel • Coagulate lining with Argon beam coagulator • ? Place omentum adjacent to exposed cyst lining
European Experience • 3 European centers (Mainz, Mannheim, Hannover) • 1995 - 2005 • 14 pts (median 8.5 yr) • 10 recurrences (71%) APSA 2006
CMH Experience1990 - 2006 • 8 pts (6 – 18 yrs) • 4 open, 4 laparoscopic • ALOS: 2.75 days (open) 1.75 days (laparoscopic) • No recurrences ( 6 CT scans)