Download
1 / 51
831 likes | 2.68k Views
Visual Evoked Potentials. M.Etemadifar Neurologist,IUMS. What is evoked potential?. Electrical potentials that occur in the cortex after stimulation of a sense organ which can be recorded by surface electrodes is known as Evoked Potential. eg. SEP, ABR and VEP . Introduction:.

E N D
VisualEvokedPotentials M.Etemadifar Neurologist,IUMS
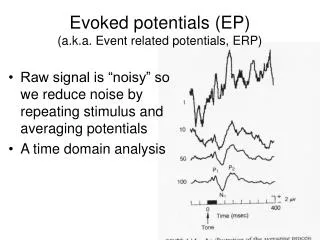
What is evoked potential? Electrical potentials that occur in the cortex after stimulation of a sense organ which can be recorded by surface electrodes is known as Evoked Potential. eg. SEP, ABR and VEP
Introduction: • The VEP tests the function of the visual pathway from the retina to the occipital cortex. • It assesses the integrity of the visual pathways from the optic nerve, optic chiasm, and optic radiations to the occipital cortex.
Cont.. • The VEP is very useful in detecting an anterior visual conduction disturbance. • However, it is not specific with regard to etiology. For example a tumor compressing the optic nerve, an ischemic disturbance, or a demyelinating disease may cause delay in the P100.
Cont… • VEPs are most useful in testing optic nerve function and less useful in postchiasmatic disorders. • In retrochiasmatic lesions, the MRI is a more useful test.
Comparison of VEP with MRI VEP • The VEP explains the functionality of visual pathway. • VEP gives us information about the physiology of a anatomical pathway with much less spatial or localizing information • VEP is useful primarily in assessing optic nerve function in the anterior (prechiasmatic) portion. • It is lateralizing but not localizing to the lesion. MRI • The MRI largely remains an imaging, structural, or anatomical test. • The MRI scan gives more accurate information about structural problems • MRI is a highly accurate localizing modality Under given circumstances they may be complementary to each other..
VEP generator site • Visual Cortex (occipital lobe) The generator site is believed to be the peristriate and striate occipital cortex .
Types of VEP • Flash VEP • Pattern VEP- • full field • hemi field • central field • partial field • Chromatic patterned stimuli-best method of separating red, green , and blue coloured channels. Helpful in detecting colour blindness.
How to do the test ? SKIN PREPARATION APPLY ELECTRODE USING JELLY RECORDING – Oz REFERENCE – Fpz GROUND – Cz ELECTRODE IMPEDANCE BELOW 5KΏ AMPLIFICATION , FILTER , SWEEP SPEED, AVERAGING TO BE CHECKED
Procedure • The room should be dark. • Test mono-ocularly with other eye covered. • Stimulus: Checkerboard pattern (or less often, flash) is used as stimulation two reversal/sec. • Stimulus rates of 1-2 Hz are recommended • The recommended recording time window (ie, sweep length) is 250 ms. • Seating distance: 70-100 cm from the monitor screen • Fix the gaze at a colored dot in the center of the screen.
Cont… • Apply three scalp electrodes at; Oz : 2cms above the inion. Cz : at vertex Fz : on frontal bone. • Check the impedance of the electrodes. • In the menu enter patient’s info (name, age , sex,ID no. ref. Dr. • Start averaging process. • Continue averaging till 1000 stimulus repetition complete. It will stop automatically.
Cont… • After the stimulus are over you will get NPN complex. • Identify the waves & apply the wave markers. the values will appear in the table. • Repeat the procedure & get another record. • Display both the recordings and superimpose them to show the reproducibility of the test results. • Repeat the procedure for other eye.
Stimulus factors & VEP • PATTERN • FIELD SIZE • DISTANCE • CONTRAST • LUMINANCE • COLOURS • RATE OF REVERSAL
Patient factors & VEP • AGE • GENDER • EYE DOMINANCE • VISUAL ACUITY • PUPILLARY SIZE • ALERTNESS
Factors influencing VEP • The size of the checks • Pupillary size • Gender (women have slightly shorter P100 latencies ), and • Age: below 1 yr of age P100 may be 160ms, & above 60 yrs. also it get delayed. • Sedation and anesthesia abolish the VEP. • Visual acuity deterioration up to 20/200 does not alter the response significantly . • Drugs.(eg. carbamazepine and sodium valproate prolong P100 latency)
REFERENCE RECORDING GROUND
Analysis • Identify the waves (NPN complex) • Determine the absolute peak latencies. • Determine the amplitude of the waves. • Determine the interocular latency difference.
Interpretation • Negative components of NPN complex may be absent even in normal subject. The only persistent wave is P100.
N75 N145 P100 Waveforms(The NPN complex) • The initial negative peak (N1 or N75) • ِA large positive peak (P1 or P100) • Negative peak (N2 or N145)
Delayed P100 is due to, 1. Demyelination of optic nerve. 2. Axonal degeneration. • Low voltage of P100 is due to, Problems of refrective medias of eye. eg. Corneal opacity, cataract , vitreous hemorrhage. • Voltage should not be less than 5mv.
Full field PVEP- criteria for abnormality Latency criteria • Prolongation > 3 sd • Interocular latency of p100>10 msec, longer latency abnormal Amplitude criteria • Interocular amplitude ratio>2 • Abnomally low or high amplitude • Absence of identifiable VEP from midline and lateral occipital sites.
Maximum Value for P100 • P100 is 110 milliseconds (ms) in patients younger than 60 years (it rises to 120 ms thereafter in females and 125 ms in males. ) (Even though published norms are available in the medical literature, each individual laboratory should have its own norms to control for lab-to-lab variability in technique. ) • Interocular P100 latency difference is upto 5 – 6 ms. > 10ms is gross abnprmality.
Flash VEP • Cortical response to flash – widespread , complex and variable • Absence is abnormal • Used in situations when PVEP not possible –ocular scarring, ocular haemorrhages • Done through closed eyes • Unaffected by refractive error • Useful in children and uncooperative patients
Chromatic patterned VEP • Best method to separate blue, red and green coloured channels • Can help in detecting color blindness
Hemifield VEP Indications • Optic chiasmal or retro chiasmal lesion • Marked interhemispheric asymmetry of VEP on monocular stimulation
Bilateral abnormal full field PVEP • Bilateral lesions in optic nerve, optic chiasm, behind chiasm, retinal degeneration, butterfly gliomas of corpus callosum.
Monocular abnormal full field VEP • Conduction defect anterior to optic chiasm • Demyelination common • retinal disease , glaucoma , compression of optic nerve cannot be excluded.
Full field PVEP interpretation • VEP normal in unilateral lesions of optic chiasm with monocular stimulation because each eye projects to both occipital lobes.
Full field PVEP interpretation • If P100 abnormality occurs in stimulation of one eye the lesion is anterior to optic chiasm i.e optic nerve, retina or other intra ocular structures.
Differential diagnosis with abnormal (prolongP100 latency) VEP • Multiple sclerosis • Optic neuropathy • Optic neuritis • Toxic amblyopia eg. Tobacco smoking, alcohol. • Glaucoma • Ischemic optic neuropathy • Tumors compressing the optic nerve - Optic nerve gliomas, meningiomas, craniopharyngiomas, giant aneurysms, and pituitary tumors • Normal VEP virtually excludes an optic nerve or anterior chiasmatic lesion.
Clinical usefulness of VEPs • More sensitive than MRI or physical examination in prechiasmatic lesions • Objective and reproducible test for optic nerve function • Abnormality persists over long periods of time • Inexpensive as compared with to MRI • Under certain circumstances, may be helpful to positively establish optic nerve function in patients with subjective complaint of visual loss; normal VEP excludes significant optic nerve disorder
Clinical applications of PVEP • Detects subclinical lesions in MS • Detects subclinical involvement of optic pathways in neurofibroma,Antibiotics • Evaluation of visual loss in hysteria, malingering • Monitoring visual functions during operations around pituitary • Confirmation of lesion of optic nerve tumour
Multiple Sclerosis (MS) • Its a chronic demyelinating disease of the central nervous system, which predominantly affects young adults during their most productive years. Viral and autoimmune etiologies are postulated. Genetic and environmental factors are known to contribute to MS, but a specific cause for this disease is not identified.
Pathologically, MS is characterized by the presence of areas of demyelination and T-cell predominant perivascular inflammation in the brain white matter. Some axons may be spared from these pathological processes • Differential diagnosis for MS includes other demyelinating diseases of the nervous system, often of a viral or postinfectious origin
PVEP in demyelination • Prolonged latency of P100 or absence of VEP during acute attack • Abnormal PVEP in 90% patients with optic neuritis • P100 prolongation persists many years – unilateral marked increase in latency with normal wave form and amplitude.
PVEP in disorders of optic nerve Ischemic optic neuritis • Invariably abnormal • Amplitude affected or absent VEP • Mild latency increase Toxins/ drugs • PVEP absent / delayed • Can revert following treatment • Used to monitor drug toxicity
PVEP in disorders of optic nerve • Compression of anterior visual pathway –decreased amplitude, distorted wave, mild latency prolongation • Leber’s atrophy, spino cerebellar degenerations –increased latency
PVEP in retinopathies • Increased latency with preservation of waveform similar to demyelination • Hence opthalmological examination mandatory in symptomatic visual loss.
PVEP in glaucoma • PVEP abnormal in 50% of patients with field defects • Increased latency with decreased amplitude of P100