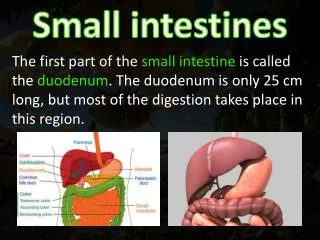
Download
1 / 32
320 likes | 609 Views
An infant with Protruding Intestines. Case Management Conference November 11, 2009. General Data. This is the case of a preterm baby boy from Sapampalay, Bulacan, delivered at PGH LRDR via low segment cesarean section to an 18 y/o G1P0 mother, presenting with protrusion of the intestines.

E N D
An infant with Protruding Intestines Case Management Conference November 11, 2009
General Data This is the case of a preterm baby boy from Sapampalay, Bulacan, delivered at PGH LRDR via low segment cesarean section to an 18 y/o G1P0 mother, presenting with protrusion of the intestines.
History of Present Illness • On the day of delivery, at 29 1/7 weeks AOG by amenorrhea, the 18 y/o G1P0 mother of the patient was referred to PGH by a local health center for control of preterm labor. Ultrasound was done revealing gastroschisis. Dexamethasone 1 dose IM was given to the mother and a live baby boy was delivered via low segment cesarean section for gastroschisis, 35 weeks by pediatric aging, 1550 grams, SGA. Tactile stimulation, suctioning, and thermoregulation were done and APGAR scores were noted to be 9,9.
Family Medical History No family history of asthma, allergy, DM, hypertension, PTB, cancer No family history of any congenital anomalies
Personal and Social History The patient was born to an 18 y/o G1P0 mother, who is single, unemployed, High School undergraduate, with no vices nor pollution exposures. The father of the patient is a 19 y/o unemployed, elementary graduate, heavy smoker, and occasional alcoholic beverage drinker.
Maternal History The mother of the patient had her first coitus when she was 17 y/o with 1 NPSP. She had no comorbidities nor illnesses during gestation. She had regular PNCU since 3 months AOG c/o a local health center. She took multivitamins and FeSO4 as advised to her. She denies intake of any antibiotic and teratogens nor exposure to radiation.
Physical Examination at Birth • Patient was received stable, acrocyanotic with good cry, good activity, good muscle tone • HR 140, RR 40, afebrile • Anictericsclerae, pink conjunctivae, formed nose, ears, lips, tongue and palate • Equal chest expansion, no retractions, clear breath sounds • Adynamicprecordium, no precordial bulge, distinct heart sounds, normal rate and regular rhythm, no murmurs
Physical Examination at Birth Abdomen with ~7x8 cmwall defect with erythematous and edematous bowels protruding lateral to the umbilical cord without sac Grossly male genitalia with descended testes Full and equal pulses, acrocyanotic, no clubbing, no edema
Initial Assessment Preterm, 35 weeks by pediatric aging, 1550 grams, small for gestational age, cephalic presentation, delivered via primary low segment cesarean section for gastroschisis, live baby boy, APGAR 9,9 Gastroschisis Rule out Sepsis
Differential Diagnosis Omphalocoele Congenital herniation of abdominal contents at the umbilicus into the umbilical cord. Amniotic sac (amnion & peritoneum) is always present but it may have ruptured at or before birth exposing the contents.
Differential Diagnosis Gastroschisis Full thickness abdominal wall defect situated almost always to the right of the umbilicus without a covering membrane. A bridge of skin separates it from the umbilicus.
Differential Diagnosis Umbilical Cord Hernia Congenital herniation of abdominal contents at the umbilicus into the umbilical cord with less than 4 cm in size. Amniotic sac is present but it may also have ruptured at or before birth exposing the contents.
Differential Diagnosis Prune Belly Syndrome Congenital deficiency of abdominal musculature, urinary tract dilatation and cryptorchidism
Course First Day of Life • Diagnostics including CBC, blood CS, blood typing and babygram APL were done. • Started on Meropenem (40) and Amikacin (15). Patient was placed on NPO with IVF D10W at 9.5cc/hr (TFI 150) • Patient was brought to the OR for SILO closure of gastroschisis and right IJ cutdown. Findings at operation include edematous, erythematous bowels, abdominal defect extending superiorly and inferiorly. • Patient was intubated ET 3, level 7.5, maintained on MV settings: FiO2 60%, PIP 20, PEEP 5, RR 40, IT 0.4.
Course Second Day of Life Patient was started on albumin (1) 25% to run at 8cc for 24 hours with furosemide while on albumin. Noted to have no urine output. Inotropes Dopa (5) and Dobu (8) were started to enhance renal perfusion. TFI was increased to 200 cc/kg.
Course Third Day of Life PPN was started at D10 Na3 K2 Ca400 AA0.5. Weaning from mechanical ventilator was started. Patient was able to tolerate weaning and was eventually extubated.
Course 8th Day of Life Awaiting second stage closure. Patient was started on Fluconazole (12) and Ciprofloxacin (20).
Final Diagnosis Preterm, 35 weeks by pediatric aging, 1550 grams, small for gestational age, cephalic presentation, delivered via primary low segment cesarean section for gastroschisis, live baby boy, APGAR 9,9 Gastroschisis Rule out Sepsis
Definition Herniation of bowel loops & other abdominal organs through a defect in the abdominal wall w/ no associated covering /sac Defect just to the right of the umbilical cord
Epidemiology strongly associated with very low maternal age More frequent in primipara Associated w/ low social economic status Poor maternal education Drug abuse (alcohol,cigarettes,cocaine) may have vasoreactive effects during embryo development baseline birth prevalence is 1 in 50,000 births and has increased since between 10- and 20-fold.
Demographic occurs in approximately two infants per 10,000 live births in the United States and internationally. Mothers below the age of 20 are birth to affected babies. Gastroschisis occurs slightly more often in males than in females. four times as likely as mothers in their late twenties to give
Demographic Maternal intake of aspirin or ibuprofen causes 4 to 5 times increased risk for gastroschisis. Both medications are inhibitors of the cyclooxygenase enzyme and influence blood flow to the fetus. Decongestants, especially pseudoephedrine and phenylpropanolamine,double the risk (cause constriction of blood vessels and decrease blood flow to the fetus) Illness and fever have no association with the development of gastroschisis.
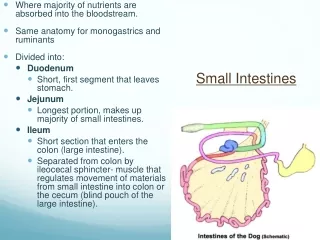
Embryology During the 4th week of development, the lateral body folds move ventrally and fuse in the midline to form the anterior body wall. Incomplete fusion defect that allows abdominal viscera to protrude through the abdominal wall. The bowel typically herniates through the rectus muscle, lying to the right of the umbilicus.
Signs & Symptoms A mother carrying a fetus with gastroschisis will not experience any unusual signs or symptoms in early pregnancy. suspected when maternal serum screening reveals an elevated AFP level (not indicative of gastroschisis specifically, but this does alert for a detailed ultrasound)
Diagnosis Ultrasonogram the primary method of diagnosis (noninvasive, rapid, and allows for real-time fetal monitoring) May reveal: -loops of fetal intestines floating exposed to amniotic fluid w/ or w/o other organs -signs of intestinal obstruction -defect in the middle of the abdominal wall to the right of a normal umbilical cord. Diagnose gastroschisis before 20 weeks of gestation Transvaginal Sonogram diagnosis has been made as early as 12 weeks of gestation. AFP levels elevated maternal serum AFP level is present in approximately 75 to 80% of cases
Diagnosis Upon birth radiographs and bowel contrast studies may be necessary to diagnose intestinal complications.




![STOMACH, INTESTINES, RECTUM [SURGICOSE]](https://cdn4.slideserve.com/8061806/medical-instruments-medical-instruments-dt.jpg)