Download
1 / 54
540 likes | 707 Views
CVD RISK WITH METABOLIC SYNROME and DIABETES. James R. Sowers, M.D. Professor of Medicine , Physiology and Pharmacology Director, Diabetes and Cardiovascular Research Center University Of Missouri Medical Center,Columbia,Missouri. Over the next 24 hours:.

E N D
CVD RISK WITH METABOLIC SYNROME and DIABETES James R. Sowers, M.D. Professor of Medicine , Physiology and Pharmacology Director, Diabetes and Cardiovascular Research Center University Of Missouri Medical Center,Columbia,Missouri
Over the next 24 hours: • 2200 diabetics will be newly-diagnosed • 512 diabetics will die • 66 diabetics will go blind • 77 diabetics will be diagnosed with ESRD • 153 diabetes-related amputationsi Source: American Diabetes Association
45 40 Men (n=4265) Women (n=4559) 35 30 25 20 15 10 5 0 20-29 30-39 40-49 50-59 60-69 70 ? Metabolic Syndrome: Prevalence Increases With Age 47 million or 23% of US Adults Have Metabolic Syndrome Prevalence, % Age, yr Adapted from: Ford ES, et al. JAMA. 2002;287:356-359.
What Causes the Rising Incidence of Diabetics and the metabolic syndrome in the USA and Other Countries?
Is It Gluttony or Sloth?? Jack in the Box Bacon Ultimate Cheeseburger 1020 Calories 71 grams of Fat Average American child or teen watches 3-4 hoursTV per day
FRENCH(Freedom ?) FRIES 20 Years Ago Today 210 Calories 2.4 ounces 610 Calories 6.9 ounces How many calories are in these fries? Calorie Difference: 400 Calories How to burn* 400 calories: Walk 2 hr 20 Minutes *Based on 130 pound person
Pneumonia/Influenza Other MalignantNeoplasms 5% 4% 13% 55% 13% 10% Diabetes STROKE Heart Disease Causes of Mortality in Patients With Diabetes Diabetes in America.. NIH No. 95-1468. 1995:233-257.
CV Events in People With Diabetes: Framingham Heart Study – 30-y Follow-up 10 Men 9 Women 11 Risk ratio 19 30 38 9 6 3* 20 Total CVD CHD Cardiac failure Intermittent claudication Stroke Age-adjusted annual rate/1,000 P < .001 for all values except *P < .05 Wilson PWF, Kannel WB. In: Ruderman N et al, eds. Hyperglycemia, Diabetes, and Vascular Disease. Oxford; 1992.
Changing Rate of Stroke • Stroke rates are not falling • Incidence level or increasing • Similar to CHF and atrial fibrillation • May be due to increased DIABETES rates • Increasing number of elderly with advanced vascular disease • Increasing incidence + aging population = 20%-40% increase in the number of strokes/y
Adverse Prognostic Implications of Cardiovascular Metabolic Syndrome Population-based observational study in 1209 men Metabolic syndrome present Metabolic syndrome absent Coronary heart disease mortality Cardiovascular disease mortality All-cause mortality RR (95% CI): 3.77 (1.74-8.17) RR (95% CI): 3.55 (1.96-6.43) RR (95% CI): 2.43 (1.64-3.61) Cumulative Hazard (%) Follow-up (years) Follow-up (years) Follow-up (years) Lakka H-M et al. JAMA. 2002;288:2709-2716.
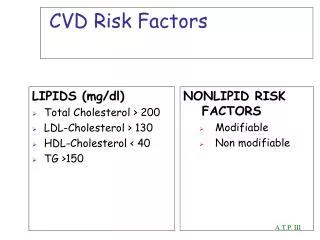
JNC 7: CVD Risk Factors • Hypertension* • Cigarette smoking • Obesity* (BMI >30 kg/m2) • Physical inactivity • Dyslipidemia* • Diabetes mellitus* • Microalbuminuria • estimated GFR <60 ml/min • Age (older than 55 for men, 65 for women) • Family history of premature CVD (men under age 55 or women under age 65) *Components of the metabolic syndrome. JAMA 2003:289:2560
Impaired Endothelium-Dependent Vasodilation in People at Risk for Type 2 Diabetes 16 13.7 12 10.5 9.8 8.4 8 % Increase over baseline of brachial artery diameter 4 0 Relatives** IGT Diabetes Control 1st-Degree relatives *C vs R, IGT, D **1 or both parents Caballero AE et al. Diabetes. 1999; 48: 1856-1862.
Lumen Lumen Cytokines TNF IL-1 IL6 Liver Endothelial Cells Endothelial Cells Markers of Inflammation & Thrombosis “Vulnerable” plaque ActivatedAdipocytes, T-Lymphocytes, Macrophages Endothelial Cell Activation PAI-1 t-PA ICAM, VCAM selectins CRP SAA Gabay C, NEJM 1999; 340: 448 Libby P, Circulation 1999; 100: 1148
Central obesity Insulin resistance Triglycerides HDL-C (Small Dense LDL particals) Absent nocturnal drop in BP/HR Microalbuminuria coagulation/fibrinolysis Increased Inflamation (NASH)(fatty liver) ROS Generation CV (Metabolic) Risk Factors in Diabetics Linked to Vascular Dysfunction CV Oxidative Stress/ Impaired Endothelial Function Sowers J,Haffner S: Hypertension2002.
CHD Mortality According to Risk-Factor Status 140 120 100 80 60 40 20 0 Non-Diabetic Diabetic CHD Death Rate* per 10,000 Person-Years None One Two Three Risk Factors *Age adjusted Stamler et al, Diabetes Care 1993
How can we reduce the CVD risk in persons with Cardiometabolic Syndrome@ Diabetes Mellitus?
Strategies for Reducing Macrovascular Complications Prevention proven by intervention • Dyslipidemia • Hypertension • Antiplatelet therapy Prevention suggested by epidemiology • Disorders of Thrombolysis • Endothelial disorders • Inflammation/Oxidative Stress
Association of SBP and CVD Death in Type 2 Diabetes 250 Non-diabetic 225 Diabetic 200 175 150 Cardiovascular Mortality Rate/10,000 Person-Yr. 125 100 75 50 25 0 < 120 120 -139 140 -159 160 -179 180 -199 > 200 Systolic Blood Pressure (mm Hg) Stamler J, et al. Diabetes Care. 1993;16:434-444.
Association of SBP and CVD Death in Type 2 Diabetes 250 Non Diabetic 225 Diabetic 200 175 150 Cardiovascular Mortality Rateper 10,000 Person-Years 125 100 75 50 25 0 <120 120–139 140–159 160–179 180–199 ≥200 Systolic Blood Pressure (mmHg) Stamler J et al. Diabetes Care. 1993;16:434–444.
Tight BP Control vs Tight Glucose Control Microvascular Any DM Stroke DM Death Complications End Point 0 –10 - –20 - Reduction in Risk (%) –30 - Tight Glucose Control –40 - Tight BP Control *P < 0.05 –50 - UKPDS Group. BMJ. 1998:317;703–713.
25 20 15 10 5 0 HOT: Greatest Benefit at ≤80 mmHg in Diabetes and Hypertension * *P = 0.005 24.4 * 18.6 Events per1,000 Patient-Years 11.9 ≤90 mmHg ≤85 mmHg ≤80 mmHg Hansson L et al. Lancet. 1998;351:1755–1762.
Multiple Antihypertensive Agents are Needed to Achieve Target BP Trial Target BP(mmHg) No. of antihypertensive agents 1 2 3 4 McFarlane1BP 130/85 ABCD DBP <75 MDRD MAP <92 HOT DBP <80 AASK MAP <92 UKPDS DBP <85 DBP=diastolic blood pressure; MAP=mean arterial pressure. Bakris GL et al. Am J Kidney Dis. 2000;36:646–661. 1. McFarlane SI et al. Diabetes Care. 2002;25;718–723.
Key Points for Optimal Hypertension Management <140/90mm Hg <130/80 mm Hg in diabetes or renal disease JNC 7BPGoals • JNC 7 recommends: • If SBP >20 mm Hg, DBP >10 mm Hg over goal, • consider initiating with 2-drug combination JNC 7 Report. Hypertension. 2003;42(6):1206-1252. 28
Other Glomerulonephritis 10% 13% No. of patients Diabetes Hypertension Projection 27% 95% CI Diabetes: Most Common Cause of ESRD Primary Diagnosis for Patients Who Start Dialysis 700 600 50.1% 500 No. of dialysis patients (thousands) 400 520,240 300 281,355 200 243,524 100 r2=99.8% 0 1984 1988 1992 1996 2004 2000 2008 United States Renal Data System. Annual data report. 2000.
Central obesity Insulin resistance Low HDL cholesterol levels High triglyceride levels Small dense LDL particles Systolic hypertension Salt sensitivity Elevated CRP & other inflammatory markers Absent nocturnal drop in BP/HR Increased CV oxidative stress Impaired endothelial function Abnormal coagulation/ fibrinolytic profiles Left ventricular hypertrophy CVD Risks that Cluster with Microalbuminuria • Microalbuminuria Sowers and Haffner Hyp. 2002
Proteinuria Is an Independent Risk Factor for All-cause Mortality in NIDDM Normoalbuminuria (n=191) Microalbuminuria (n=86) Probability of Survival Macroalbuminuria (n=51) P<0.01 normoalbuminuria vs microalbuminuria and macroalbuminuria P<0.05 microalbuminuria vs macroalbuminuria Years Gall MA et al. Diabetes. 1995;44:1303-1309.
Metabolic Syndrome/CKD Defined • Metabolic syndrome is defined as the presence of 3 or more of the following risk factors • HTN • low HDL-C • high triglycerides • elevated glucose • abdominal obesity • CKD is defined as estimated GFR below 60 mL/min/1.73 m2, microalbuminuria(30 mg/g creatinine ) Chen et al. Annals Intern Med. 2004;140:167-174.
Metabolic Syndrome and Chronic Kidney Disease/Microalbuminuria in US Adults • Metabolic syndrome is a common risk factor for CVD • Cross sectional analysis of NHANES III • Patients greater than 20 years of age, CKD (n=6,217), microalbuminuria (n=6,125) • Metabolic syndrome as previously defined • CKD as previously defined Chen et al. Annals Intern Med. 2004;140:167-174.
Multivariate Odds Ratio for CKD or Microalbuminuria Based on Presence of Components of the Metabolic Syndrome Chen et al. Annals Intern Med. 2004;140:167-174.
Greater Benefit on CV Events with in Patients with Renal Insufficiency in HOPE . *P<0.05 * * * Hazard ratio Primary outcome MI Stroke CV death All death Hosp HF Revasc Mann JE et al.Ann Intern Med 2001
Microalbuminuria Overt Proteinuria Doubling of Creatinine End Stage Renal Disease Progression of Renal Disease CV Events Death
BP(ACE/ARB)- Reduction for Renal Protection Hemodynamic Effects • Reduction in systemic BP • Reduction in glomerular capillary pressure because of efferent glomerular arteriolar dilation • Reduction in proteinuria Nonhemodynamic • Inhibition of macrophage/monocyte infiltration • Reduction in Inflammation • Reduction in Oxidative Stress
Biochemical Results(AllHAT) * p<.05 compared to chlorthalidone † Ann Intern Med. 1999;130:461-470
Development of Diabetes in ALLHAT *p<.05 compared to chlorthalidpone
18 16 14 12 10 8 6 4 2 0 VALUE: Incidence of New-onset Diabetes 23% Risk Reduction With Valsartan P < 0.0001 New-Onset Diabetes (% of patients in treatment group) 16.4% 13.1% Valsartan-based Regimen (n = 5094) Amlodipine-based Regimen (n = 5074) Julius S, et al. Lancet. 2004;363:2022-2031.
HOPE/HOPE-TOO: Development of diabetes New Diabetes - All Patients HOPE Study Ends 0.12 Ramipril 0.10 Placebo 0.08 Hazard 0.06 0.04 ALL: RR: 0.69, CI: (0.57-0.83) 0.02 CONT: RR: 0.70, CI: (0.57-0.86) 0.0 Years 1 2 3 4 5 6 7 Bosch J. European Society of Cardiology C 2003. Vienna, Austria
LIFE: New-Onset Diabetes Intention-to-Treat 0.10 0.09 Atenolol (N=3979) 0.08 Losartan (N=4019) 0.07 0.06 End Point Rate 0.05 0.04 0.03 0.02 Adjusted Risk Reduction 25%, P<.001 Unadjusted Risk Reduction 25%, P<.001 0.01 0.00 Study Month 0 6 12 18 24 30 36 42 48 54 60 66 Dahlöf. 2002.
0.1 0.2 0.5 1 2 5 10 Favors Treatment Favors Control Prevention of Type 2 Diabetes by Inhibition of the RASResults • StudyTreatment Control RR (fixed) 95% CI RR (fixed) 95% CI ALLHAT 2002 119/5840 302/9733 ALPINE 2003 1/196 8/196 CAPP 1999 227/5184 280/5229 CHARM 2003 163/2715 202/2721 HOPE 102/2837 155/2883 LIFE 2002 241/4006 319/3592 SCOPE 2003 99/2160 125/2170 SOLVD 2003 9/153 31/138 STOP-HTN-2 1999 99/1969 97/1961 .66 [0.53, 0.81] 0.13 [0.02, 0.97] 0.09 [ 0.70, 1.03] 0.01 [0.66, 0.97] 0.69 [0.52, 0.85] 0.75 [0.64, 0.88] 0.81 [0.62, 1.06] 0.26 [0.13, 0.53] 0.95 [0.72, 1.26] Total (95% CI) 25060 29023 Total events 1158 (Treatment), 1609 (Control) Test for heterogeneity Chi2 =22.39, df = 8 (p = 0.004), P = 64.3% Test for overall effect Z = 6.73 (p < 0.00001) 0.78 [0.72, 0.84] Scheen A. Diabetes 2004;53(S2);A169.
DREAM NAVIGATOR • Valsartan • Nateglinide 2#2
Steno-2: Multifactorial Intervention on Macro and Microvascular Outcomes 160 patients with type 2 diabetes/microalbuminuria Conventional therapy 53% risk reduction P=0.01 Composite CVD outcome* (%) Intensive therapy† Follow-up (months) Conventional therapy better Intensive therapy better *CV death, MI, stroke, revascularization, amputation †Total fat intake <30%, >30% min excersise 3-5 x weekly, ACE inhibitor, ASA, BP <130/80 mm Hg, total-C <175 , TG <150 mg/dL, A1c < 6.5% N Engl J Med. 2003;348:383–1393.
Prevention of CVD in Diabetes • No Smoking • ASA • Lipid Control (Statin) + LDL <70, HDL >45-50, TG <150 mg/dl (HMG CoA Reductase Inhibitors) • Blood Pressure <130/80 mm Hg • Glycemic Control: A1C<7% • Dash Diet and increased Aerobic Excercise
Metabolic factors associated with CVD in postprandial state Endotheial Dysfunction Platelet activation Fibrinolytic resistance coagulability Postprandial Glycemia Postprandial lipemia
Ins/IGF-1 receptor Glucose Transport PO4 MAP kinase AKT IRS-1 (-) P13-K Na-K ATPase NOS gene / expression & incresed glucose transport (-)ROS? (+) Mitogenesis, hypertrophy & remodeling Ang II
25 20 15 10 5 0 VA-HIT: Increasing HDL-C Reduces Risk of CV Death RRR 22% (95% CI, 7-34; P=.006) Placebo Cumulative incidence (%) Gemfibrozil 0 1 2 3 4 5 6 Year Rubins HB et al. N Engl J Med. 1999;341:410-418.
ANG II - SUPEROXIDE PRODUCTION IN HUMAN VASCULATURE. Human Internal Mammary Arteries incubated with Angiotensin II 02- * p< 0.01 N = 11 N = 11 N = 15 . Ang II Ang II + ARB CONTROL Circ. 2000;101:2206-2212