Download
1 / 38
430 likes | 589 Views
Fever in Children. Jay Hescock M.D. Assistant Professor of Pediatrics LSU Department of Pediatrics. Objectives. Review etiologies of fever without a localizing source in the pediatric population

E N D
Fever in Children Jay Hescock M.D. Assistant Professor of Pediatrics LSU Department of Pediatrics
Objectives • Review etiologies of fever without a localizing source in the pediatric population • Discuss appropriate evaluation and treatment of children presenting with fever without a localizing source • Discuss preliminary data and the possible implications of universal pneumococcal immunization on the work-up/treatment of fever without a localizing source
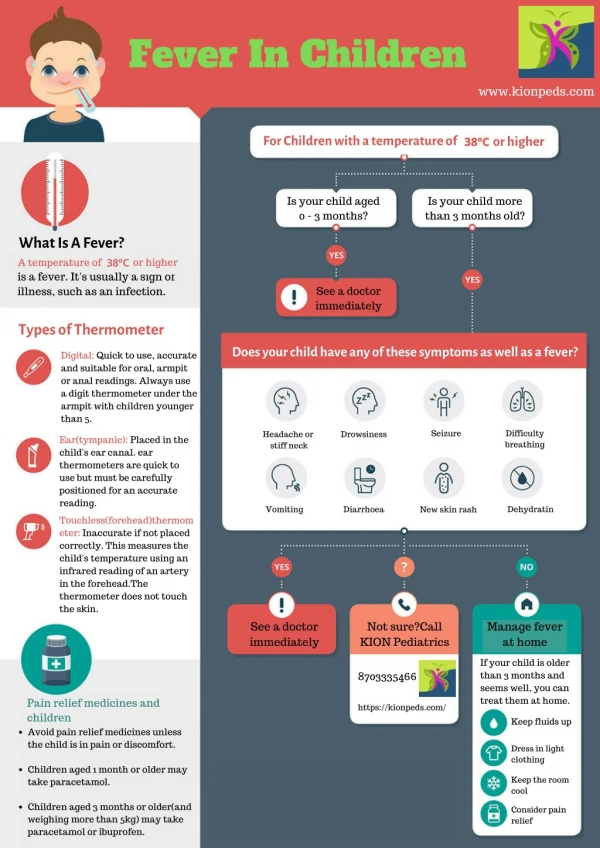
Measuring Fever • Rectal - most reliable in infants under 3 mos • Oral - only reliable in cooperative children • Axillary - least invasive; less accurate • Tympanic - results variable. Generally 1.0 to 1.8 F lower than rectal temperature • Pacifier - requires 3 to 4 minutes. Generally 0.5 F lower than rectal temperature • Temperature of 38 C (100.4 F) or greater considered fever
Fever Without a Localizing Source Refers to an acute febrile illness in which the etiology of the fever is not apparent after a thorough history and physical exam
Etiology of Acute Fever Without Localizing Source • Infants < 28 days • Serious Bacterial Illness (UTI, bacteremia/sepsis, meningitis, pneumonia, bone/joint), viral infections • Infants 1 to 3 months • SBI, viral infections • Children 3 to 36 months • Occult bacteremia, SBI, viral infections
Definition of Toxicity • Refers to the apparent severity of a child’s disease based on physical exam • Yale Observation Score (not always reliable in young infants) • Child’s cry, reaction to parents, state variation, response to social overtures, color, hydration status • Clinical picture consistent with sepsis syndrome (with or without fever!) • lethargy, poor perfusion, hyper/hypoventilation, or cyanosis
Evaluation of the Toxic Child • Complete blood count • Blood cultures from 2 sites • Urinalysis • Urine culture • CSF studies, including culture • Consider unique factors eg. central lines, indwelling catheters/hardware
Treatment of the Toxic Child • Neonates <3 months: Ampicillin (high dose) + an aminoglycoside (or 3rd generation cephalosporin). Consider anti-staphylococcal coverage if warranted on PE • Children > 3 month: Vancomycin + 3rd generation cephalosporin • **Antibiotic coverage should be narrowed as soon as susceptibilities are known**
1993 Practice Guideline - Rochester Criteria - Fever Without Localizing Source • Infants < 28 days old • Hospitalize • Full sepsis work-up with blood/urine/CSF cultures • IV antibiotics with ampicillin and 3rd generation cephalosporin or gentamicin to cover common pathogens in this age group (GBS, E. coli, and Listeria) • antibiotic may be D/C at 48-72 hours provided cx (-) and child remains well appearing
1993 Practice Guideline - Rochester Criteria - Fever Without Localizing Source • Infants 28 to 90 days old • Low risk • Option 1: BCx, UCx, outpt observation without antibiotics, re-evaluate in 24 hours • Option 2: BCx, UCx, CSF cx, outpt observation with Ceftriaxone x 1, re-evaluate 18 to 24 hours • Non low risk • Hospitalize, blood/urine/CSF cultures, IV abx
Low Risk Criteria - Rochester 1993 • Previously healthy • Non-toxic appearing • No focal bacterial infection on examination • Negative laboratory screening • WBC 5,000 to 15,000 • Less than 1,500 absolute band count • Normal urinalysis • Less than 5 WBC/hpf in stool if diarrhea present
Results - Rochester • Infants < 90 days • 1.1% low risk had bacteremia • 1.4% low risk had serious bacterial infection • 0.5% low risk had meningitis • Sensitivity 83-97% • Specificity 47-53% • PPV 10-16% • NPV 97-100%
Summary – Infants < 3 months old • Infants < 28 days should be fully evaluated and treated for possible SBI, since clinical and laboratory criteria are not reliable indicators of SBI • Infants 29 to 90 days should have laboratory evaluation and treatment according to protocols. LP should be done if antibiotics are given. Low risk infants may be safely managed as outpatients if parents are reliable
1993 Practice Guideline - Rochester Criteria - Fever Without Localizing Source • Children 3 to 36 months old (nontoxic) • Fever < 39.0 C (102.2 F) • No laboratory tests or antibiotics • Return if fever persists >48 hour or clinical picture deterioration
1993 Practice Guideline - Rochester Criteria - Fever Without Localizing Source • Children 3 to 36 months old (nontoxic) • Fever > 39.0 C (102.2 F) • WBC < 15,000 and UA normal – no additional tests, supportive treatment • return if fever persists >48 hours or clinical picture deteriorates • WBC > 15,000 • Blood culture, stool culture if bloody diarrhea • Urine culture for boys < 6 months, girls < 2 years • Ceftriaxone pending culture results • Re-evaluation 24 to 48 hours
Occult Bacteremia • Definition: Positive blood culture in a well-appearing febrile child (clinically indistinguishable from those without bacteremia) • Most cases occur between 6 and 24 months; may occur as early as 3 months • Can occur with common bacterial illnesses such as otitis media
Incidence of Occult Bacteremia in Children with FWLS • Before routine H. influenzae vaccination • 3 to 11% • 85% S. pneumoniae • 10% H. influenzae • 3% N. meningitidis
Incidence of Occult Bacteremia in Children with FWLS • After routineH. influenzae vaccination • 1 to 5% • >90% S. pneumoniae • remainder: N. meningitidis, Salmonella species, group A streptococci, and S. Aureus
1993 Practice Guideline - Recommendation for Treatment • Children 3 to 36 months with positive BCx • H. influenzae or N. meningitidis - hospitalize, repeat BCx, lumbar puncture, IV antibiotics • S. pneumoniae • Afebrile and well appearing - 2nd dose Ceftriaxone, then 10 days oral penicillin • Febrile or ill appearing - hospitalize, lumbar puncture, IV antibiotics pending sensitivities
Rochester Criteria - Results Using Practice Guideline 1993 • Guidelines do not totally eliminate all risk as the NPV of a WBC <15, 000 is 97% • Children 3 to 36 months • Without outpatient antibiotics 20% with occult bacteremia will have persistent bacteremia • 9.2% developed meningitis (3-4/1000) • With outpatient antibiotics 4% with occult bacteremia will have persistent bacteremia • 4.5 % developed meningitis (2/1000) • Highlights the need for appropriate F/U
Occult Bacteremia in Children with FWLS The Current Era - After S. pneumoniae vaccination
Pneumococcal Vaccine • Licensed in 2000 • Protein-polysaccharide conjugate vaccine • Targets 7 serotypes commonly associated with invasive pneumococcal disease (causing 80% IPD) • When started as infant, involves 4 shot regimen
Impact of Pneumococcal Vaccine • Black et al. (PIDJ 2000) • 94% effective in reducing disease caused by vaccine serotypes • 89% reduction in invasive pneumococcal disease regardless of serotype • Whitney et al. (NEJM 2003) • 78% reduction in disease caused by vaccine related serotypes • overall 69 % reduction in invasive disease regardless of serotype
Impact of Pneumococcal Vaccine • Fireman et al. (PIDJ 2003) • 11% decrease in pneumonia • 7.8% reduction in visits for OM and 5.7% reduction in antibiotic prescriptions • Kaplan et al. (Pediatrics 2004) • 77% reduction in disease caused by vaccine related serotypes • 66% reduction in invasive disease overall
Impact of Pneumococcal Vaccine • Stoll and Rubin (APAM 2004) • incidence of occult bacteremia in children 2-36 months old with temp >39C was 0.91% • neither elevated total WBC >15,000 or elevated ANC was highly predictive of occult bacteremia • Hsu et al. (PIDJ 2005) • 69% reduction in IPD since introduction of PCV7
Summary - Children 3 to 36 months old • Increasing evidence that routine CBC and empiric antibiotic treatment is not necessary • UA/UCx all girls < 2y, uncircumcised boys < 2y, circumcised boys < 6 mo -1 yr (See AAP practice parameter Pediatrics 1999) • Lee et al (Pediatrics 2001) - with current rate of pneumococcal bacteremia, most cost effective method is CBC with BCx and empiric antibiotics if WBC > 15,000
Summary - Children 3 to 36 months old • Pneumococcal vaccine will decrease the incidence of bacteremia (and therefore IPD) • Full impact of vaccine on need for evaluation and empiric treatment for children with FWLS has yet to be determined • Many experts recommend continuing to use previous guidelines until full impact is assessed
Unanswered Questions • What additional effect will the new Pneumococcal vaccine have on rates of IPD • If the incidence of occult bacteremia continues to fall, will the risks associated with empiric Abx (i.e. anaphylaxis) outweigh the benefits • Are other screening tests now necessary to assess risk of SBI (i.e. procalcitonin levels) and minimize unnecessary ABX exposure
Bibliography • Alpern et al. Occult bacteremia from a pediatric emergency department: Current prevalence, time to detection, and outcome. Pediatr. 2000;106:505-510. • Bandyopadhyay et al. Risk of serious bacterial infection in children with fever without a source in the post-Haemophilus influenzae era when antibiotics are reserved for culture-proven bacteremia. Arch Pediatr Adol Med. 2002;156:512-517.
Bibliography • Baraff et al. Practice guideline for the management of infants and children 0 to 36 months of age with fever without source. Ann Emerg Med. 1993;22:1198-1210. • Baskin et al. Outpatient treatment of febrile infants 28 to 89 days of age with intramuscular administration of ceftriaxone. J Pediatr. 1992;120:22-27.
Bibliography • Black et al. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Pediatr Infect Dis J. 2000; 19:187-95. • Fireman et al. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J. 2003;22:10-16.
Bibliography • Hsu et al. Population-Based Surveillance for Childhood Invasive Pneumococcal Disease in the Era of Conjugate Vaccine. Pediatr Inf Dis J. 2005;24(1): 17-23. • AAP Practice Parameter: The diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatr. 1999;103:843-52.
Bibliography • Kadish et al. Applying outpatient protocols in febrile infants 1-28 days of age: Can the threshold be lowered? Clin Pediatr. 2000; 39(2):81-8. • Kaplan et al. Decrease of Invasive Pneumococcal Infections in Children Among 8 Children’s Hospials in the United States After the Introduction of the 7-Valent Pneumococcal Conjugate Vaccine. Pediatrics. 2004; 113(3):443-447.
Bibliography • Lee GM, Harper MB. Risk of bacteremia for febrile young children in the post-Haemophilus influenzae type b era. Arch Pediatr Adolesc Med. 1998;152(7): 624-8. • Lee et al. Management of febrile children in the age of the conjugate pneumococcal vaccine: A cost-effectiveness analysis. Pediatr. 2001;108:835-844.
Bibliography • Stoll and Rubin. Incidence of Occult Bacteremia Among Highly Febrile Youn Children in the Era of the Pneumococcal Conjugate Vaccine. Arch Pediatric Adolesc Med. 2004;158:671-675. • Whitney et al. Decline in Invasive Pneumococcal Disease after the Introduction of Protein-Polysaccharide Conjugate Vaccine. NEJM. 2003;348(18):1737-46.