Download
1 / 1
10 likes | 112 Views
*. As clinically indicated, the management options may be modified if woman is: pregnant, postmenopausal, or an adolescent. LG 43% (38/88) HG 33% (29/88). 24% (21/88). §.

E N D
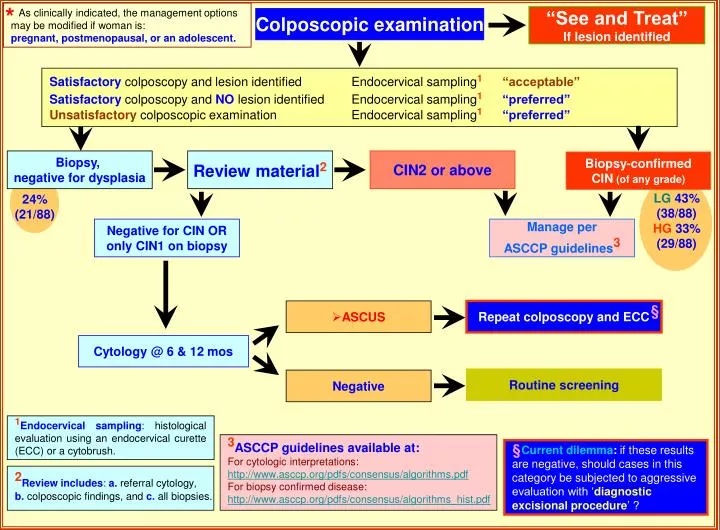
* As clinically indicated, the management options may be modified if woman is: pregnant, postmenopausal, or an adolescent. LG 43% (38/88) HG 33% (29/88) 24% (21/88) § Current dilemma: if these results are negative, should cases in this category be subjected to aggressive evaluation with ‘diagnostic excisional procedure’ ? “See and Treat” If lesion identified Colposcopic examination Satisfactory colposcopy and lesion identified Endocervical sampling1“acceptable” Satisfactorycolposcopy and NOlesion identified Endocervical sampling1“preferred” Unsatisfactorycolposcopic examination Endocervical sampling1 “preferred” Biopsy, negative for dysplasia Review material2 CIN2 or above Biopsy-confirmed CIN (of any grade) Negative for CIN OR only CIN1 on biopsy Manage per ASCCP guidelines3 § • ASCUS Repeat colposcopy and ECC Cytology @ 6 & 12 mos Routine screening Negative 1Endocervical sampling: histological evaluation using an endocervical curette (ECC) or a cytobrush. 3ASCCP guidelines available at: For cytologic interpretations: http://www.asccp.org/pdfs/consensus/algorithms.pdf For biopsy confirmed disease: http://www.asccp.org/pdfs/consensus/algorithms_hist.pdf 2Review includes:a. referral cytology, b. colposcopic findings, and c. all biopsies.