Download
1 / 65
730 likes | 1.18k Views
ADOLESCENT BRAIN DEVELOPMENT. Risky adolescent behaviors are not simply impulsive behaviors, but generally occur in the context of evaluating positive and negative consequences and immediate vs. delayed rewards (Wulfert et al., 2002)

E N D
ADOLESCENT BRAIN DEVELOPMENT • Risky adolescent behaviors are not simply impulsive behaviors, but generally occur in the context of evaluating positive and negative consequences and immediate vs. delayed rewards(Wulfert et al., 2002) • PFC activation during risk-reward conflict appears less active in adolescents compared to adults (Bjork et al., 2007)
ADOLESCENT VULNERABILITY • Adolescents who prefer immediate rewards vs delayed rewards may have underdeveloped neural circuitry for maintaining motivation and inhibiting behaviors • These adolescents may also anticipate that risky behaviors will lead to positive outcomes (Chambers et al., 2003) • Deficits in cognitive, behavioral, and emotional regulation comprise a common vulnerability for increasing risk for AUD’s
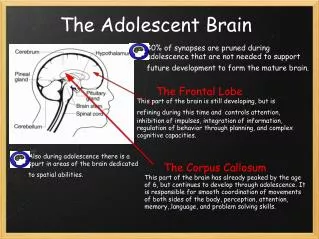
ADOLESCENT BRAIN DEVELOPMENT • With experience and PFC development, teens are able to temper their instinctive ‘gut’ reaction with more rational, reasoned responses—they are able to “apply the brakes” to emotional responses. During this time of development, teens need adult mentors and role-models who demonstrate how to make good decisions and how to control emotions
ADULT GUIDANCE • Adult monitoring is too frequently and too prematurely withdrawn during the vulnerable period leaving the adolescent to navigate difficult situations alone or with peers (Dahl,2004)
ADULT GUIDANCE • Adult thinking is guided by self regulation and delayed gratification: • Interrupting risky behavioral trajectory– “getting off a runaway train” • Thinking before acting– “jumping the gun” • Choosing between two alternative courses of action-- “doing the right thing” (Steinberg, 2004) Risk perception, internal planning, endogenous control of behavior (functions of the PFC) Steinberg, 2004)
ADOLESCENT BRAIN DEVELOPMENT • Critical developmental changes in brain pathways controlling emotions, cognitive and attentional functions, and reward sensitivity during adolescence • Strong increases in the connectivity between the amygdala (critical for emotional learning) and the PFC (critical for decision making) [Kelly, Schochet, & Landry 2004]
ADOLESCENT BRAIN DEVELOPMENT • Adolescence involves the maturation of self-regulation of behavior and emotions—teens need to learn how to navigate complex social situations under conditions of strong emotions – such as social anxieties, romances, academic pressures, immediate gratification vs long term goals, moral dilemmas, and success or failure
SCARS THAT WON’T HEAL • Growing evidence of altered brain development and functioning as the result of abuse and neglect • Our interactions with the world “organize our brain’s development” and shapes the person we become (Shore, 1997) • Brain will develop to respond to a positive or a negative environment
BRAIN ADAPTATION • Life experiences (positive or negative) set off cascades of change that influence gene expression and brain organization (Masten, 2004) • Life experiences exert a profound influence on brain architecture (Spessot, Plessen, & Peterson, 2004)
SCARS THAT WON’T HEAL • Chronic stress, abuse, and neglect sensitize certain neural pathways and over-develop certain regions of the brain (limbic region) involved in anxiety and fear. This often results in the under-development of other regions of the brain (frontal lobe) (Perry, 2000) • Chronic stress from fear, violence, abuse, hunger, pain, etc. focuses the brain’s resources on survivaland other areas of the brain are not “available” for learning social and cognitive skills
BRAIN’S RESPONSE TO THREAT • Brain is uniquely designed to mobilize the body in response to threat—all body response—fight or flight • Neurochemical systems cause a cascade of changes in attention, impulse control, sleep patterns, and fine motor control (DeBellis, 2001) • Chronic activation of the neural pathways involved in fear creates “memories” which shape a person’s perception of and response to the environment—indelible perception of the world (attitudinal change?)
BRAIN’S RESPONSE TO STRESS • PFC is extraordinarily sensitive to stress. Even mild stressors can impair PFC cognitivefunctioning if the person feels no control over the stressor (frequent in teens) • High levels of Dopamine are released during stress – this impairs the regulation of thought and behavior – may explain why teens are vulnerable to loss of judgment and insight during emotional or stressful situations (Arsten & Shanksy, 2003)
GENDER DIFFERENCES IN RESPONSE TO STRESS • Corticosterone response to stress differs in male and female rats (in females-greater overall response, faster rise in blood levels, and blood levels binding increased) [Young & Altemus, 2003] • Estrogen may amplify many aspects of the stress response – significant implications for our understanding of depression and anxiety in females
STRESS AND LEARNING • Hormones involved with the HPA axis have profound influence on brain circuits that are integral to learning, memory, emotional regulation, and behavioral affect(Cameron, 2003) • Neurobiological factors that amplify stress-induced PFC dysfunction during adolescence, may increase susceptibility to impaired judgment, substance abuse, and psychiatric disorders (Arsten & Shanksy, 2003)
NEUROBIOLOGY OF ABUSE • Chronic activation of certain parts of the brain involved in the fear response - hypothalamic-pituitary-adrenal-(HPA) axis can “wear out” other parts of the brain such as the hippocampus (memory, cognition, communication) • HPA axissignificantly influences cognitive development as well as behavioral and emotional regulation • Abuse and addiction impact learning, behavior, and psychological and moral development on a cellular level (issue of choice?)
JANUARY22, 2007 A CHILD HOLDS A WEAPON IN A BAGHDAD PROTEST IN DECEMBER, 2006
NEUROBIOLOGY OF ABUSE • Chronic stress may have neurotoxic effects and lead to learning and concentrationimpairments secondary to the damage to the hippocampus including: -- accelerated loss of neurons (Smythies, 1997) -- delays in myelination (Dunlop, 1997) -- abnormalities in developmentally appropriate pruning (Todd, 1992) -- inhibition of neurogenesis (Tanapat, 1998)
Child Abuse and Neglect OUTCOMES PTSD Symptoms in Childhood Compromised Cognition & Psychosocial Effects Alterations of the Catecholamine & HPA Axis Changes in Brain Metabolism (enhanced neuron loss, anterior cingulate dysfunction) Adverse Effects on Brain Development (smaller cerebellum, corpus callosum) De Bellis, 2001
THE EFFECTS OF ABUSE AND NEGLECT • Diminished growth in the left hemisphere — may increase risk for depression(Teicher, 2000) • Irritability in the limbic system can set the stage for the emergence of panic disorder and post-traumatic stress disorder (Teicher, 2000) • Smaller growth in the hippocampuscan increase the risk for dissociative disorders and memory impairment(Teicher, 2000)
Cognitive problems Anxiety Suicidal ideation Depression Attention problems Attachment problems Impulsive behavior Aggression Acting out Antisocial behaviors Persistent fear Hyper-arousal Dissociation Disrupted attachments Lack of empathy Sleep problems Tachycardia Hypertension Memory problems Explosive anger CLINICAL PRESENTATION (Perry, 2000)
More Adolescents Use Alcohol Than Use Cigarettes Or Marijuana Percent The Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking, 2007
Adolescents Drink Less Often But More Per Occasion Than Adults Usual number of drinks/occasion Drinking days/month The Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking, 2007
Among Adolescents Who Drink, The Number Of Binge Drinking Days Increases With Age Days Age The Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking, 2007
18-20 Year Olds Have The Highest Prevalence Of DSM-IV Alcohol Dependence Percent Age The Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking, 2007
Alcohol Use and Binge Drinking Vary by Race/Ethnicity and Gender Percent Gender and Racial/Ethnic Subgroups Source: SAMHSA, Office of Applied Studies, NSDUH (special data analysis)
ALCOHOL AND ADOLESCENTS • Alcohol is the drug of choice among America’s adolescents – used more than tobacco or illicit drugs (Johnson et.al., 2006a) • Underage drinking is deeply embedded in our culture – many view it as a “rite of passage” • Parents can influence a teen’s thinking about drinking • A substantial number of adolescents begin drinking at a very young age and this often occurs at home – this increases their chances of developing an alcohol use disorder
ALCOHOL AND ADOLESCENTS • Nearly 1/3 of American youth begin drinking before age 13 (Grunbaum et.al., 2004) • The peak years for alcohol initiation are 7th & 8th grades (Faden, 2006) • Underage drinking contributes to serious adolescent health and social problems including: death from injuries, risky sexual behaviors (Cooper & Orcutt, 1997), increased risk of physical & sexual assault (Hingson et al., 2005), and academic failure (Grunbaum et al., 2005) • Parents need to talk to their teens about drinking and set specific no-use expectations
ALCOHOL AND ADOLESCENTS • The developing adolescent brain may be particularly vulnerable to negative effects from alcohol (Brown, et al., 2000; Crews, et al., 2000 De Bellis, et al., 2000) • Youth with school, personal, or family problems are more likely to begin drinking early (Brown & Tappert, 1999) • Youth who begin drinking prior to age 14 have a 41% chance of developing alcohol dependence during their lifetime compared with those who wait until age 21when lifetime risk is reduced to 10%(Brown & Tappert, 1999)
ALCOHOL AND ADOLESCENTS • Hippocampus (memory area of the brain) is sensitive to the acute effects of ethanol during adolescence (White and Swartzwelder, 2004) • Hormonal fluctuations, differences in metabolism, & gender specific drinking patterns may account for the mounting evidence that female teens suffer greater alcohol related problems than male teens
ALCOHOL AND ADOLESCENTS • Compared with controls, adolescents with AUDs have been found to have smaller prefrontal white matter volumes (DeBellis, 2005) • Some research has suggested that adolescents and adults with AUDs have smaller amygdala, hippopocampal, and ventral striatum volumes than controls (Koob, 1999; Mill et al., 2001; Makris et al., 2004) • Implications for reward sensitivity, inhibition, impulsivity, and decision making
ARE ADOLESCENTS MORE SUSCEPTIBLE TO ALCOHOL THAN ADULTS? • Adolescent rats are LESS sensitive to the aversive effects of alcohol such as sedation, hang over, & motor impairment effects (consequently they may drink more than adults)[Doremus et al., 2003; Varlinskaya & Spear, 2004] • Adolescent rats are MORE sensitive to the social disinhibition induced by alcohol use (consequently they feel the “stimulating/fun” aspect of drinking sooner than adults) [Doremus et al, 2003; Varlinskaya & Spear, 2004]
ALCOHOL’S EFFECTS • Family characteristics, such as history of alcoholism, psychopathology, gender, and age of first use, must be carefully considered when studying the influence of teen drinking on cognition(Brown & Tappert, 2004) • Extensive literature suggests that COAs (children of alcoholics) exhibit verbal, non-verbal, and memory deficits on cognitive tests (Hill, 2004)
ALCOHOL’S EFFECTS • Alcohol use during adolescence may “lock in” the insensitivity to alcohol’s sedative effects (Varlinskaya & Spear, 2004; White & Swartzwelder, 2004) • Changes in the neurochemical components of insensitivity may raise the hedonic (pleasure seeking) set point leading to compulsive alcohol and drug use (Hill, 2004)
ALCOHOL EXPECTANCIES • Alcohol expectancies form early and shift over time: 3-5 year olds associated alcohol with neutral, adult behavior 9-10 year olds associated alcohol with negative, wild, dangerous behavior 10-12 year olds associated alcohol with more positive, fun behavior Windle et al., 2008
INHIBITORY CONTROL PFC ACG REWARD Hipp MEMORY/ LEARNING NAcc VP Amyg Brain Circuits Involved in Drug Addiction OFC SCC MOTIVATION/ DRIVE (saliency)
One mechanism contributing to addiction may be the ability of drugs to induce damage in the nucleus acumbens –impacting the serotonin and dopamine neuromodulator systems (both implicated in impulsivity) –further promoting impulsive choices and drug taking behaviors(Cardinal, Winstanley, Robbins, & Everitt, 2004)
CONTROL CIRCUITS • fMRI studies demonstrate abnormalities in the PFC– area for decision making and inhibitory control • These abnormalities could be involved in the changes in decision making, judgment, and cognitive control that occur in addiction • Changes in the PFC could lead to loss of self-directed/willed behavior in favor of automatic sensory driven behavior(Goldstein and Volkow, 2002)
ADOLESCENTS AND ALCOHOL • Underage alcohol use is a highly complex problem • Biological, social, familial, cultural, genetic, & environmental factors all contribute to an adolescent’s decision to use alcohol • Parents, schools, governments, and the entire community need to be involved in prevention underage drinking
PROGRAMMING AND POLICY ISSUES • Teensare not adults –BRAIN development is not complete • Teens operate from the emotional, impulsive, reward oriented part of the brain • Communication is a complicated process • Technology is transforming the world • Disparities between knowing/feeling & understanding/behaving
PROGRAMMING AND POLICY ISSUES • Adolescent alcohol use is influenced by the availability, price, cultural and subcultural norms, adult monitoring (schools, family, law enforcement), and peers as well as individual motives, desires, expectancies, values, and vulnerabilities (Masten et al., 2008) • Prevention and treatment interventions must address the physical, relationships, cultural groups, and media/virtual contexts that adolescents live in
PROGRAMMING AND POLICY ISSUES • Teens need strong, consistent social scaffoldingstructures/people that provide support, guidance, constraints, monitoring, encouragement, & a safety net (Dahl, 2004) • Emergence of teen regulatory skillsrequires a solid, consistent foundation and maturation of the PFC (Masten, 2004)
PREVENTION INTERVENTIONS Domain: family, school, neighborhood, peers, workplace, policy, or multiple domains Target Population: adolescent, parents, siblings, peers, or community Type of Strategy: universal, selective, or indicated Most successful strategies are multi-component which place emphasis on increasing parenting skills and increasing adolescent regulatory capacity
PREVENTION INTERVENTIONS • Consider including strategies addressing: alcohol expectancies, peer/sibling use (everybody does it) hot/cold situational role plays impulse/inhibition activities strategy/team activities group problem solving activities
DEVELOPMENTAL PROCESSES/TRANSITIONS THAT MAY AFFECT RESPONSES TO PREVENTION OR TREATMENT INTERVENTIONS
TREATMENT INTERVENTIONS • Most treatment interventions are “borrowed” from adult treatment system • Adolescent focused treatment can be effective • Maturation of PFC and limbic system including self-regulation, executive function, and cognitive capacity, as well as family conflict, depression, and aggression need to be considered and addressed in treatment