Download
1 / 30
300 likes | 314 Views
This study explores the potential of using monocytic stem cells derived from peripheral blood to generate neoislet cells for the treatment of diabetes. The characterization and differentiation of these cells were examined in vitro, and markers of neoislet cells were analyzed. Glucose challenge tests and insulin and C-peptide assays were performed to evaluate the functionality of the neoislet cells.

E N D
Generating Neoislet Cells from Stem Cells of Monocytic Origin
Mahgoub M.A., M.D Pancreatic Islet Transplantation and Diabetes Researches Unit. Ain Shams University, Cairo, Egypt.
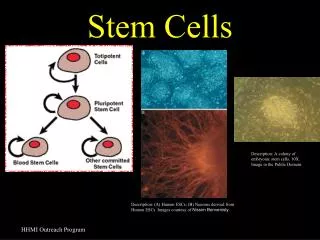
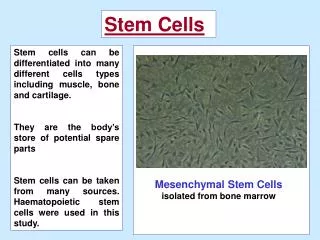
Background The demand for islet cells for treatment of diabetes and lack of pancreata and the problem of immunosuppression with the allogenic transplantation directed our thoughts towards stem cell therapy. Stem cell therapy can be defined as group of new techniques or technologies that relay on replacing diseased or disfunctioning cells with healthy functioning one.
Stem cells could be obtained from human fetuses, umbilical cords, or embryonic tissues derived from fertilized eggs. However these sources of stem cells raise ethical and legal questions, pose a risk of transmitting infections, and/or may be ineffective because of immune rejection.
Aim of The Work In the present study, we have described the characterization and differentiation in vitro of a subset of human peripheral blood monocytes that behave as stem cell. The ability to obtain these stem cells from an easily accessible source such as peripheral blood should make them valuable candidates for autologus transplantation.
Material and Methods I- Generation of Neoislet Cells . Mononuclear layer was obtained from peripheral blood of healthy donors by density gradient centrifugation and further purified by MACS technology to obtain monocytes [Miltenyi Biotic - Germany]. The purity of the monocytes was tested by flow cytometry analysis of CD14 , also CD34 was done.
Monocytes are then cultured for 6 days in dedifferentiation culture media; RPMI 1640 based medium containing 10% fetal calf serum,L-glutamine, penicillin , streptomycin and specific growth factor: macrophage colony stimulating factor (M-CSF), human interleukin 3 (IL3). These cells are now termed programmable cells of monocytic origin (PCMO) and flow cytometry analysis for CD14 and CD34 was performed again. PCMO were then cultured in islet cell conditioning medium [ICM] containing epidermal growth factor, hepatocyte growth factor, nicotinamide and glucose for 21 days to be differentiated into neoislet cells.
II- Analysis of Neoislet Cells. After 7,14 and 21 days differentiated PCMO were subjected to real time RT-PCR and immunohistochemistry. Glucose challenge test was done on day 21 and insulin and C-peptide were assayed by radioimmunoassay .
RESULTS I. Flow Cytometry Analysis: Monocytes were tested by flow cytometry before culturing for CD14 and CD34. They showed that CD14 (specific for monocytes) was (82% + 6%) and CD34 ( marker of stem cell) was (0% + 3%) . II. Neoislet Cell Markers by RT-PCR: We confirmed neoislet differentiation by real time RT-PCR at day 7, 14 and 21 of culturing in ICM for common islet cell markers; β - actin, Pdx-1, insulin and glucagon.
At day 7 (as shown in fig 1),weak amplification signal for β - actin and Pdx-1 was detected. No insulin or glucagon expression was found. After 14 days we got good amplification signals for Pdx-1, insulin and glucagon gene. While after 21 days (as show in fig2) maximum expression of gene Pdx-1, β - actin, insulin and glucagon was found. ( We found no amplification signals for Pdx-1, insulin , glucagon in PCMO which was used as control).
Weak Signal for ß-actin Weak Signal for Pdx-1 After 7 Days in ICM Culture
Pdx-1 gene expressed in our Total Reference RNA, HUMAN Insulin gene expressed in our Total Reference RNA, HUMAN Glucagon gene expressed in our Total Reference RNA, HUMAN ß-actin gene expressed in our Total Reference RNA, HUMAN After 21 Days in ICM Culture
III. Immunohistochemistry : Neoislets cells were subjected to immunohistochemistry against insulin and glucagon. In day 7 positive staining for glucagon (as shown in fig 3) and negative for insulin was found while positive for both insulin and glucagon in day 21 (as shown in fig 4a & 4b). Immunohistochemistry staining was found to be negative for both insulin and glucagon in PCMO.
On Day 7 After Culture in ICM Positive Staining for Glucagon and Negative for Insulin
Positive For Both Insulin and Glucagon On Day 21 After Culture in ICM Insulin Glucagon
IV. Results of Insulin and C – Peptide: Supernatant collected from the glucose challenge performed to the neoislet cells was assayed by RIA for insulin and C-peptide. The results showed that insulin was (3.2, 5.7 and 6.8 µIU/ ml) and C-peptide results were (0.8, 1.4 and 1.5 ng/ml) for glucose concentrations: 50, 300 and 400 mg/dl respectively. (as shown in fig 5).
IV. Results of Insulin and C – Peptide After Glucose Challenge Insulin C-peptide
DISCUSSION In the present study, the in-vitro differentiated monocytes derived neo-islet cells resembles primary human counterpart in several aspects: 1- Genetic Markers of Neoislet Cells by real time RT-PCR showed expression of Pdx-1 which is a regulatory gene important for β-cell function detected early after 1 week of culture in ICM. Real time RT-PCR analysis of our results revealed endogenous de novo expression of insulin and glucagon at high amplification signals at day 21 of ICM culture.
2- Immunohistochemichal assay in our work provides positive glucagon granules at day 7 in ICM while at day 21, it provides positive results for both insulin and glucagon which mimics the normal embryological development of the islet cells. As during embryonic life, β-cells are recognized 2 weeks after alpha cells development. 3- Metabolic Function by performing glucose challenge test , Neoislet cells appears to resemble pancreatic islet cells in metabolic activity by secreting insulin and C-peptide in a glucose dependent fashion.
Animal Model Aim of The Work: Autologus implantation of Neoislet Cells generated from stem cell of monocytic origin in canine. Methods and Results: Preparation of Dogs Seven male mongrel dogs were chosen. 6 dogs were prepared for implantation and 1 for control. Each dog was subjected to single IV injection of alloxan to induce diabetes.
Generation of Neoislet Cells : 30 ml of peripheral blood was taken from each dog separately . The peripheral blood monocytes were cultured for 28 days by the above technique to generate neoislets cells. Implantation : Six dogs were injected by neoislet cells suspended in 1 ml ICM in the deltoid muscle and injected between the muscle fibers. The seventh dog (control dog) was injected by 1 ml ICM only. All dogs were off of insulin at the day of implantation.
Evaluation of graft function A- Fasting Blood Glucose of (FBG) of 3 dogs were normalized. The FBG of 4th and 5th dogs were ameliorated; the 4th didn’t need insulin (135 + 5 mg/dl) while the 5th dog need a small dose of insulin (200 + 5 mg/dl). The 6th dog died one day after implantation and the cause of death was unexplained. FBG of the control dog remained high. B- To Assess The Ability of the implanted dogs for glucose load disposal, an oral glucose tolerance test was performed for the first 4 dogs.
3 dogs showed normal pattern of oral glucose tolerance curve. The 4th dog showed a pattern of impaired glucose tolerance.
C- Immunohistochemistry After 50 days, the grafts were removed from all dogs for immunohistochemical study. In the 5 recipient dogs, the cells were viable and showed the presence of positive insulin and glucagon granules between the muscle fibers as shown in fig (7a and 7b). The graft of the control dog was negative for both insulin and glucagon granules.
DISCUSSION In our study, autologus implantation of neo-islet cells into diabetic dogs was capable of regulating or ameliorating blood glucose level post implantation up to 50 days Despite that the intramuscular implantation might not be the ideal site for islet implantation, it has been chosen for its high neovascularization capability and its easy accessability (*). (*) Mahgoub M, Ammar A., Ashmawi H., Akl M., Hammam O. The deltoid muscle could be a suitable site for islet transplantation 2005; poster presentation in the 10th IPITA congress, Geneva, Switzerland.
After removal of the graft from the deltoid muscle, the dog recurred to hyperglycemic state as pre implantation compared to the control diabetic dog which remained hyperglycemic throughout the study.
Conclusion The most exciting perspective in this study is the potential use of stem cell of monocytic origin for treatment of diabetes mellitus. In possible future clinical applications, islet cells may first be generated in vitro and upon autologus transplantation into patients may substitute for their endogenous counterparts.