Download
1 / 37
370 likes | 571 Views
Cooperation Bilharz-Beaujon Cairo - March 16-18, 2008. PVT In Patients With Chronic Liver Disease. Dominique-Charles Valla Hôpital Beaujon, APHP, Université Paris-7, Inserm CR3B. PVT in Patients with Cirrhosis. Epidemiology Manifestations Causal factors Therapy.

E N D
Cooperation Bilharz-Beaujon Cairo - March 16-18, 2008 PVT In Patients With Chronic Liver Disease Dominique-Charles Valla Hôpital Beaujon, APHP, Université Paris-7, Inserm CR3B
PVT in Patients with Cirrhosis Epidemiology Manifestations Causal factors Therapy
Prevalence of Overt PVT in Cirrhosis Screening for HCC 0.6 % In-Hospital 7.0 % Necropsy 8.0 % Before LTx or PSS 15.0 % Okuda et al. Gastroenterology 1985;89:279-86. Chang et al. J Pathol Bacteriol 1965;89:473-80.
18% pt/yr Listed for liver transplantation Sclerotherapy 12% pt/yr Incidence of PVT in Patients with Cirrhosis Amitrano, Endoscopy 2002. Francoz et al. Gut 2005
Prevalence of Occult PVT in Cirrhosis Liver explants % Veins involved Small mural thrombus 64 % Large veins (intimal fibrosis) 25 % Small veins (intimal fibrosis) 36 % Wanless et al. Hepatology 1995;21:1238-47.
Prevalence of Overt PVT in Schistosomiasis Preoperative 5 % Splenectomy/Devascularization 19 % Distal splenorenal shunt 50 % Widman. Hepatogastroenterology 2003
PVT in Patients with Cirrhosis Epidemiology Manifestations Causal factors Therapy
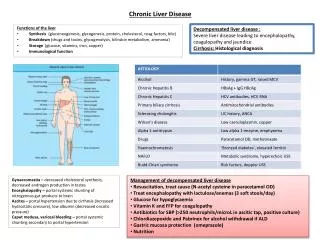
PVT and Cirrhosis: Associations • Portal hypertensive bleeding • Failure to control bleeding • Ascites • Hepatic encephalopathy • Hyperdynamic circulation • Intestinal ischemia or infarction Nonami Hepatology 1992. Orloff J Gastrointest Surg 1997. D’Amico Hepatology 2003. Amitrano J Hepatol 2004.
PVT and Cirrhosis: Associations At LTx N Liver weight • PVT 63 17 g/Kg • No PVT 401 21 g/Kg P < .02 Nonami et al. Hepatology 1992;16:1195-8
Advanced Liver Disease Thrombosis Decreased Portal Blood Inflow Blood stasis Wall changes (PHT) Advanced Liver Disease Thrombosis
PVT in Patients with Cirrhosis Epidemiology Manifestations Causal factors Therapy
Causes For Venous Thrombosis Local factors External Factors Environmental THROMBOSIS Internal Factors Prothrombotic Disorders Inherited Acquired
Inherited Prothrombotic Disorders Gain of function Factors (FV, FII) Common (> 2.0%) Moderate risk Dg: DNA analysis Loss of function Inhibitors (PC, PS, AT) Uncommon (< 0.1%) High risk Dg: Plasma level
Acquired Prothrombotic Disorders Common Moderate risk Inflammatory states Malignancy Hyperhomocysteinemia … Uncommon High risk Myeloproliferative dis. APL syndrome PNH Behcet’s disease …
Inherited Prothrombotic Disorders Gain of function Factors (FV, FII) Common (> 2.0%) Moderate risk Dg: DNA analysis Loss of function Inhibitors (PC, PS, AT) Uncommon (< 0.1%) High risk Dg: Plasma level
Coagulation Inhibitors in Cirrhosis 75% 50% 0% 100% Child-Pugh B A C A B C B C B C A A Antithrombin Protein C Protein S Romero-Gomez. J Clin Gastroenterol 2000
Acquired Prothrombotic Disorders Common Moderate risk Inflammatory states Malignancy Hyperhomocysteinemia … Uncommon High risk Myeloproliferative dis. APL syndrome PNH Behcet’s disease …
PVT and Cirrhosis: Antiphospholipid Ab • ACL common in chronic liver diseases (20%) • Usually non specific (low fluctuating titer, no LA) Mangia, Am J Gastroenterol 1999. Dalekos, Eur J Gastro Hepato 2000. Munoz-Rodriguez, J Hepatol 1999. Prieto, Hepatology 1996. Quintarelli, J Hepatol 1994. Violi, Hepatology 1997. Romero-Gomez J Clin gastro 2000
Risk Factors for Portal Vein Thrombosis. Cirrhosis without HCC Univariate: Age, Child-Pugh class, Surgery for portal hypertension Endoscopic sclerotherapy Prothrombotic features Mangia, Am J Gastroenterol 1999. Nonami, Hepatology 1992. Davidson, Transplantation 1994. *Amitrano, J Hepatol 2004.
p With PVT No PVT PVT and Cirrhosis: Prothrombotic Disorders NS < .05 < .05 < .01 7 % 2 % 5 % F. V Leiden F. II gene mutation C677T MTHFR At least one Two or more 13 % 35 % 43 % 70 % 22 % 14 % 0 Amitrano et al. Hepatology 2000;31:345-8.
Risk Factors for Portal Vein Thrombosis. Cirrhosis without HCC Univariate: Age, Child-Pugh class, Surgery for portal hypertension Endoscopic sclerotherapy Prothrombotic features Multivariate: G20210A FII (OR 5.94*) Mangia, Am J Gastroenterol 1999. Nonami, Hepatology 1992. Davidson, Transplantation 1994. *Amitrano, J Hepatol 2004.
PVT in Patients with Cirrhosis Epidemiology Manifestations Causal factors Therapy
PVT and Cirrhosis: Why to treat? • To prevent aggravation ? • To facilitate transplantation
Portal Vein Thrombosis Clinical results of anticoagulant therapy • In patients without cirrhosis • In patients with cirrhosis
60 40 Recanalization (%) 20 0 0 3 6 9 12 15 18 Time to recanalization (months) Acute PVT: Complete Recanalization Pts at risk:
Chronic Portal Vein Thrombosis Anticoagulation Anticoagulation yes yes no no 17 6.0 p = 0.212 per 100 patients per year p = 0.015 7 1.2 Bleeding Thrombosis Condat et al. Gastroenterology 2001; 120:490
Chronic portomesenteric venous thrombosis Warfarine no yes 1.00 HR for Death p=0.038 0.10 Orr et al. Hepatology 2005; 42: 212A (AASLD San Francisco 2005)
Patients on the Waiting List for LTx PVT before transplantation (n = 29) No anticoagulation (n = 10) Anticoagulation (n = 19) Recanalization (n = 8) Recanalization (n = 0) Francoz, Gut 2005
TIPS for PVT in Cirrhosis • Limited data • Feasible and safe • Risk of obstruction unclear • Risk of encephalopathy unclear • Benefit unclear Senzolo Alim Pharmacol Therap 2006. Van Ha Cardiovasc Intervent Radiol 2006. Bauer Liver Transplant 2006
PVT and Cirrhosis: Summary • Common in end-stage cirrhosis • Uncommon in well-compensated cirrhosis • Causal factors: surgery, stasis, thrombophilias • A marker for severity: certainly • A cause for aggravation: uncertain • A limitation for liver transplantation: certainly
PVT and Cirrhosis: What we do in Beaujon Objectives: Recanalization (recent thrombus) Prevention of thrombus extension Indications: → Child A with thrombophilia → Patients listed for LTx Monitoring: Anti-Xa 0.5 U/ml Factor II 25% to 35%
Hemostasis in Cirrhosis • Normal thrombin generation in platelet-poor plasma. • Decreased thrombin generation in severely thrombocytopenic blood. • Elevated levels of vWF support platelet adhesion despite reduced functional capacities. Caldwell. Hepatology 2006
INR in Patients with Cirrhosis • Not related to prothrombin levels along the same regression line as for Vitamin K antagonists. • Due to uncarboxylated metabolites of coagulation factors • Interlaboratory variability. → Adjustment based on Factor II level 25-35%?
Patients on the Waiting List for LTx PVT before transplantation 24 Partial 21 Complete 3 Recanalization 0 Recanalization* 15 * No post-OLT PVT Francoz, ILTS 2008
Acute Portal Vein Thrombosis Recanalisation 83% 75 % Thrombolysis (in situ, n = 20) Anticoagulation (alone, n = 27) Condat. Hepatology 2000 Holliingshead. J Vasc Interv Radiol 2005
Acute Portal Vein Thrombosis 100 Major Bleeding % 60% 5% 0 Thrombolysis (in situ, n = 20) Anticoagulation (alone, n = 27) Condat. Hepatology 2000 Holliingshead. J Vasc Interv Radiol 2005