Download
1 / 18
190 likes | 329 Views
Participant Questions. 1. Concurrent anti-platelet therapy with VKA or LMWH?. VTE Wild Card: Two Studies You May Have Missed. Matthew Rondina, MD University of Utah. Statin’s Effects May Extend to the Red Thrombus of VTE. JUPITER Study Design. N=17,802 healthy men and women

E N D
Participant Questions 1. Concurrent anti-platelet therapy with VKA or LMWH?
VTE Wild Card:Two Studies You May Have Missed Matthew Rondina, MD University of Utah
JUPITER Study Design • N=17,802 healthy men and women • LDL < 130 mg/dL and hs-CRP ≥ 2.0 mg/L • Randomized to rosuvastatin 20mg daily or placebo • Median FU: 1.9y (max 5 yrs) • Occurrence to first VTE protocol-specified secondary endpoint • Intention-to-treat analysis Glynn RJ et al. N Eng J Med 2009;360:1851-61
Rosuvastatin 20mg Daily Reduced Risk of First VTE Glynn RJ et al. N Eng J Med 2009;360:1851-61
Effect Consistent Across Subgroups • Similar to reduction in arterial events • No association with LDL, HDL, TG, hs-CRP • Similar reductions for provoked and unprovoked VTE • No significant difference on early vs late events (>24 mos) • Effect consistent across subgroups • Gender • Age • BMI, waist circumference • Metabolic syndrome Glynn RJ et al. N Eng J Med 2009;360:1851-61
Expands role of statins for 1º VTE prevention Unknown if any benefit for 2º prevention May be statin-specific + Rosuva, ? + Simva No effect with pravastatin Suggested, but unproven, uses: VTE prophylaxis in cancer 2º prevention where AC is contraindicated Should Statins Be in the Water? N Eng J Med 2009;360:1851-61 JTH 2004;2:700-1 JTH 2004;2:695-6 JTH 2006;4:1925-7
In Search of the Holy Grail in Acute Sub-Massive PE:Can We Further Refine Our Ability to Risk Stratify?
Pulmonary Embolism May Lead to Sudden Cardiovascular Collapse Acute PE Pulmonary HTN RV Function RV Volume LV under-filling: hypotension RV Pressure Micro-infarction Shear Stress
Hypotension Normal BP, + RVD/RVE Normal BP Nl biomarkers No RVD/RVE
Clinical Risk Stratification for Acute PE: Geneva Risk ScorePE Severity Index Cancer Age Heart failure Male Sex Previous DVT Cancer Systolic Pressure <100 Heart Failure pa02 < 8 kPa Chronic lung disease DVT on US Pulse rate >100/min Systolic Pressure <100 Resp Rate >30/min Temp < 36 degrees C Altered mentation Sa02 <90% Low Risk30d mortality GRS 84% 5.6% PESI 36% 0.9% Arch Intern Med 2006;166:169-175 JIM 2007; 261:597 CHEST 2007; 132:24 Thromb Haem 2008; 99:502
Pulmonary Embolism: Biomarker-Based Risk Stratification Natriuretic PeptidesTroponin I/T Mortality ?? 5-fold PPV 12-23% 12-44% NPV 99-100% 97-100% Assay Variation Standardized Nl Range Variation Standardized Data + +++ Circ 2003;108:2191-2194 Circ 2007;116:427-433 Chest 2008;133:1531-2 Chest 2008;133:334-6 Chest 2009;136::974-982
Pulmonary Embolism:RVE Increases Mortality Risk • RV Enlargement by Echo: • Defined as a RV diameter > 90% of the LV diameter in the long axis view • Associated with 6.6% in hospital mortality (vs. 1.9%; 2.6x risk) • Associated with 47% 30-day survival (versus 71% if normal RV diameter) • When combined with elevated TnI, 30-day survival is only 25% • Noninvasive and no contrast but may not be available 24/7 in all centers Chest 2008; 133:358-362 Chest 2008;133:334-336 Am J Card 2005;96:303-305
TELESIO: Identify High-Risk APE Pts?201 Prospective, consecutive APE Pts and SBP≥90 • Clinical score: Geneva Risk Score (≥3 points) • TTE: RVE, PAP>34 mmHg, and/or RV hypokinesis* • Trop-I • Beckmann: nl<0.07 ng/mL or 20xULN • Dade: nl<0.15 ng/mLor 20xULN • BNP • Roche/Elecsys: nl<100 pg/mLor 10xULN • D-Dimer • Roche/Star: nl<250 ug/mL or 6xULN *RVD required either one or all three (restrictive criteria) J Thromb Haemost 2009;7:938-944.
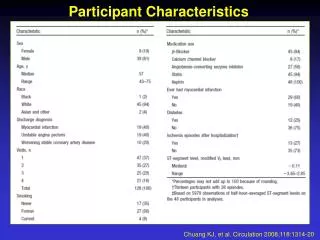
Abnormal Prognostic Markers Were Common…. J Thromb Haemost 2009;7:938-944.
But Did Not Predict In-hospital PE-related Mortality or Clinical Deterioration IP PE-Death IP All Death 3-Mo All Death [N=1, 0.5%] [2%] [9%] RVD --- --- --- RVD3 --- --- --- BNP --- --- --- BNP10 --- --- --- D-Dimer 6 --- --- + GRS* --- + + Trop-I* --- + + Trop-I 20 --- --- --- Hypoxemia --- + + J Thromb Haemost 2009;7:938-944.
3-Month Mortality Best Predicted by Clinical Score or Troponin-1 J Thromb Haemost 2009;7:938-944.
Are Prognostic Markers Useful for Identifying Higher-Risk APE for Thrombolytics? • Did not predict in-hospital PE-related AE • Did not predict 3-month PE-related mortality or VTE recurrence • May not be useful as guide to more aggressive therapy in APE with SBP ≥ 90 • Did predict 3-month all cause mortality • May reflect underlying comorbidities • Patients with normal markers had benign hospital course • Authors did not assess other outcomes • Exercise intolerance or dyspnea at rest • Persistent RV dysfunction or pulmonary HTN Bova et al, J Thromb Haemost 2009;7:938-944 Kline JA. J Thromb Haemost 2009; 7: 1601–2 Kline JA et al. Crit Care Med 2006; 34: 2773–80.