Download

1 / 13
130 likes | 242 Views
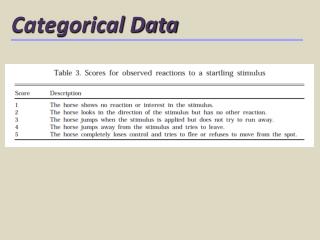
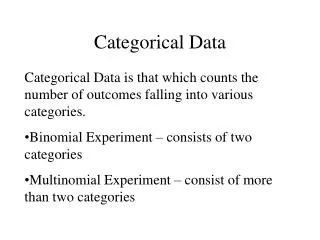
Holistic. Holistic-Content Focus: Content of an entire narrative. Holistic-Form Focus: Plots or structures of a narrative. Content. Form. Categorical-Content Focus: Content identified through content-analysis, gathered into categories. Categorical-Form

E N D
Holistic Holistic-Content Focus: Content of an entire narrative. Holistic-Form Focus: Plots or structures of a narrative. Content Form Categorical-Content Focus: Content identified through content-analysis, gathered into categories. Categorical-Form Focus: Discrete stylistic or linguistic characteristics. Categorical
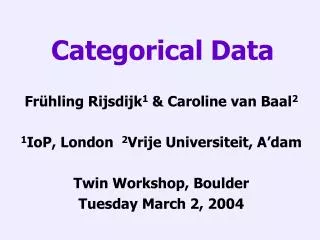
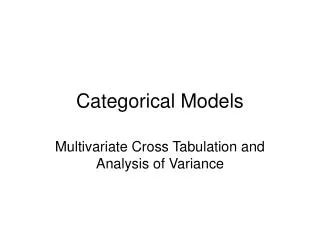
Holistic-content • Individual analysis of each case note record • Where do ill older people, being cared for in an acute hospital, want their end of life care to be provided (ideal place of care), where is it possible to provide this care (preferred place of care) and where is do they receive this care (actual place of care)? • What issues influence their ideal, preferred and actual place of care? 2. Categorical-content Collective analysis of sample 3. Categorical-form Comparison between individual and collective analyses 3. How do these issues influence preferred and actual place of care? 4. Holistic-form Construction of a narrative to illuminate the process of trying to achieve a person’s ppc. • What is the practice involved in trying to achieve ill older people’s preferred place for end of life care?
Storylines to explain facilitating ppc • Supporting the provision of care • Planning for preferred place of care • Continual assessment and review
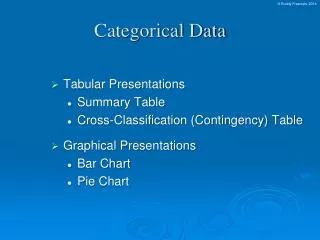
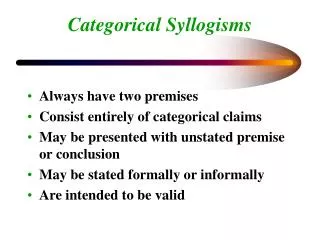
Supporting the provision of care Managing transfer from hospital to ppc or managing the person’s death in hospital Follow up with ppc Referral Assessment Agreement of ppc Continual assessment and review Follow up with hospital teams Planning ppc
Supporting the provision of care Managing transfer from hospital to ppc or managing the person’s death in hospital Follow up with ppc Referral Assessment Agreement of ppc Continual assessment and review Follow up with hospital teams Planningppc Case 82/168 (transfer to nursing home)
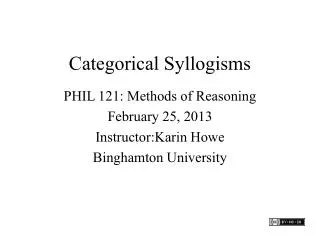
Supporting the provision of care Managing transfer from hospital to ppc or managing the person’s death in hospital Follow up with ppc Referral Assessment Agreement of ppc Continual assessment and review Follow up with hospital teams Planningppc Case 141/168 (discharge home)
Discussion questions • Has narrative enabled our clinical knowledge to be elicited? • What does it tell and not tell? • Does narrative enable this knowledge to be known by others? • How does this knowledge contribute to the research story of place of death?
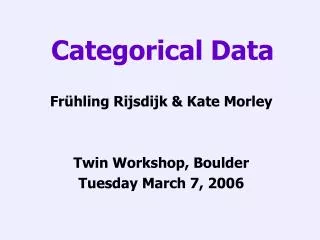
Illness factors Environmental factors Individual factors Care and place of care planning processes Illness factors not influenced or compensated by care planning and contributing to ppc not being achieved Environmental factors not influenced or compensated by care planning and contributing to ppc not being achieved Preferred place for end of life care achieved Death in hospital
Bed delay explanations • Vetting of assessment of needs • Second opinions requested • Further detail/requirements requested • Additional ppc required to be planned before accepted • Family time available to engage in selection/preferences • Waiting lists and how prioritised
Funding delay explanations • queries about a person’s needs or the level of care requested; • requiring other care options to be explored before funding would be agreed, for example, not agreeing to funding if a place was available at a hospice, irrespective of person’s preferences and needs; • caps being applied on the total amount of funding approved, for example not agreeing to a care package at home if the cost of this exceeded the weekly cost of a nursing home; • the interpretation of palliative care and which illnesses were encompassed within such care.