Download
1 / 16
160 likes | 515 Views
Paradoxical Vocal Fold Movement (PVFM). Also know as... Vocal Cord Dysfunction Vocal Cord Malfunction Laryngeal Dyskinesia Inspiratory Adduction Paroxysmal Laryngospasm Functional Airway Obstruction Adductor Laryngeal Breathing Disorder Fogerty 4/8/03.

E N D
Paradoxical Vocal Fold Movement(PVFM) Also know as... Vocal Cord Dysfunction Vocal Cord Malfunction Laryngeal Dyskinesia Inspiratory Adduction Paroxysmal Laryngospasm Functional Airway Obstruction Adductor Laryngeal Breathing Disorder Fogerty 4/8/03
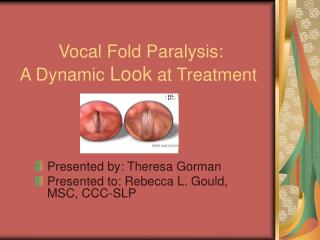
Definition Of PVFM • Inappropriate adduction of the vocal folds during inhalation • Two physiological variants: 1. Adduction of true and false folds throughout the breathing cycle 2. Adduction during deep inspiration and slight abduction on expiration
Epidemiology • incidence / prevalence unclear • may be as high as 40% of patients with asthma • age of onset: 9+ years • usually female
Etiology May be... • Coexistent with asthma • Precipitated by emotional events • Occurring with or without organic conditions (Mathieson, 2001)
Types (in order of prevalence) • Gastroesophageal reflux • Psychogenic stridor • Respiratory-type laryngeal dystonia • Drug-induced laryngeal dystonic reactions • Asthma-associated laryngeal dysfunction • Abnormalities that affect the brainstem (Koufman, 1994)
Signs & Symptoms • sensation of throat being closed • dramatic episodes of breathing difficulty • stridor • pt. struggles to inspire • shortness of breath • ‘wheezing’ • cough
Triggers • shouting or coughing • physical exercise • acid reflux • breathing cold air • irritants (smoke, pollen, etc.) • psychosocial issues • neurological issues (ASHA, 2001)
Diagnosis - History • Throat tightness • voice changes during attack • little/no improvement with asthma Tx • no night awakening secondary to attack
Physical Exam • ‘clean wheeze’ • ask pt. to pant (may improve symptoms) • ask pt. to hold breath Pulmonary • normal lung volume • relatively normal expiratory flows
Laryngoscopy • “crucial in making the diagnosis” (Koufman, 1994) Classic Pattern • VF adduction of anterior two-thirds during inspiration • Posterior glottal chink during closure on inspiration • 50% will have normal VF motion when asymptomatic
Laryngoscopic Examination • alternatively phonate /i/ and sniff, rapidly • take deep breaths • cough, throat clear, chuckle • count to fifty, rapidly and loudly • read a written passage in a loud voice • sing (Koufman, 1994)
Differential Features (Koufman, 1994)
Confused Diagnoses • Asthma • Other causes of laryngeal obstruction • bilateral vocal fold paralysis • laryngeal stenosis Abduction may be inconsistent, incomplete, inappropriate in PVFM, but must occur for a diagnosis Many patients have inappropriately received intubation or tracheostomy. Sometimes multiple times!
Behavioral Treatment • Understanding anatomy and physiology of the laryngeal system • learn to control vocal fold movement • Performing relaxation exercises • differential relaxation of excess tension in upper body • Focusing • focal breathing on face rather than neck • Reducing precipitators • daily log to chart precipitators of PVFM episodes
Additional Treatment • Heliox - 80% helium, 20% oxygen • relieves most severe symptoms • Psychological intervention