Download
1 / 19
260 likes | 1.36k Views
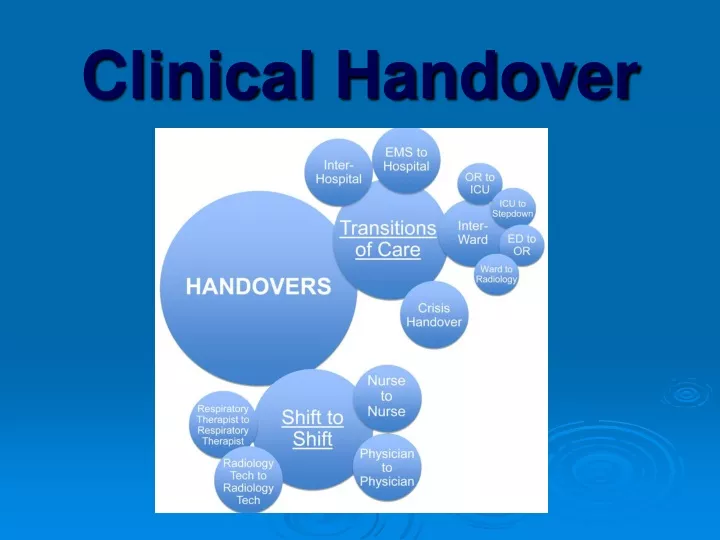
Clinical Handover. Interest and momentum in handover improvement is growing rapidly throughout the healthcare system: in all jurisdictions, in local health areas, in educational institutions and among front-line clinicians. Importance of clinical handover.

E N D
Interest and momentum in handoverimprovement is growing rapidly throughout thehealthcare system: in all jurisdictions, in localhealth areas, in educational institutions andamong front-line clinicians.
Importance of clinical handover • Clinical handover is a high risk area for patient safety • An Australian study of emergency department handover found that in 15.4% of cases, not all required information was transferred, resulting in adverse events (Ye et al, 2007). • Patient care is complex. One element of this complexity is the number of contacts and transitions undertaken by patients
What is clinical handover • Clinical handover is the transfer of professional responsibility and accountability for some or all aspects of care for a patient, or group of patients, to another person or professional group on a temporary or permanent basis.
The negatives • Failures in clinical handover have been identified as a major preventable cause of patient harm. • Poor handover can also lead to wasted resources. • Consequences include: unnecessary delays in diagnosis, treatment and care; repeated tests, missed or delayed communication of test results; and incorrect treatment or medication errors.
All clinicianscan improve their own handover practice, buthandover is a group practice and to ensurepatient safety, we need to improve the handoverpractices of all staff.
PACU HANDOVER In PACU (post anaesthetic care room) we use ISBAR to guide our clinical handover practices
At the start of clinical handover1. Staff introduce and identify themselves to each other2. Staff introduce and identify the patient with confirming 3 points of identity-NameDate of birthUR number
PAPERWORK AND DOCUMENTATION ORDER FOR HANDOVER FROM PACU • Anaesthetic pre assessment sheet • Identify patient • Identify procedure • Patient medical background history including physiological and surgical, pre existing medical conditions and identification of other relevant information i.e. alerts- infection control precautions, psychological factors (anxiety), lifestyle –IVDU (intravenous drug user) • Regular medications • Allergies • Premedication if given
2. Anaesthetic report Type of anaesthetic given and airway device used if applicable and location of regional drug administration Medications administered in the order they were administered (Ensure handover of narcotics, anti emetics and antibiotics given as they are most likely to be administered during ongoing post operative patient care) Fluids and infusions administered Stable/unstable, vital signs, discuss any events, including respiratory or cardiac events and interventions Fluid loss including blood and urine (IDC for spinal patients).
3. Surgeon report Discuss surgical procedure undertaken Any complications of procedure Any implantable devices or remaining items such as drains and packs Local infiltrated Post operative orders and instructions including diet, observations, mobilisation, limb elevation and post operative testing including bloods and x-rays Check wound sites, drains and PV loss with nursing staff as applicable at handover
4. Perioperative nursing report Should contain documentation for type of dressing used size of drains and catheters types of packs and size and if impregnated with solutions or drugs type of local and amount used any other drugs used such as dye, contrast and antibiotics etc
5. PACU report Airway on arrival and alterations during PACU admission and ongoing O2 requirements (PCA etc) Patient progression and complications with emphasis on post operative pain and nausea Medications (Ensure handover of narcotics, anti emetics and antibiotics given as they are most likely to be administered during ongoing post operative patient care) Stable/unstable, vital signs, discuss any events, including respiratory or cardiac events and interventions Fluids and infusions administered Fluid loss including blood and urine (IDC for spinal patients), any reinforced or changed dressings Discuss where relevant, DVT prophylaxis, BSL and management, PCA, dermatone level, airvo Inform of Q-ADDS, CEWTS or QMEWT score and any other anaesthetic instructions including variances for these
6. Medication chart Handover medications ordered and ensure medications for ongoing care which have already been administered within the perioperative setting have been signed Ensure antibiotics are ordered if required Ensure medications for pain and nausea are ordered where appropriate Ensure purple label is placed on medication form for exclusion of further narcotics within 24hrs following spinal anaesthesia containing Morphine
7. Fluid order chart Ensure ongoing fluids are ordered where appropriate i.e. PCA, nausea and vomiting, dextrose solutions with insulin infusions and blood products if required post operatively Oxytocin order as required
8. ADDS, CEWTS, QMEWTS Ensure form is completed with a set of observations for PACU and the score is recorded at the bottom. Ensure total score is not greater that 3 and any single score of 2 or greater is discussed with the relevant anaesthetist and documented. Variances should only be made for chronic conditions Inform staff receiving patient of total score and any variance that may have been made.
9. Other paperwork where relevant PCA (order and observation forms) BGL forms Blood or x-ray request forms Medical certificates Airvo order
Resources QHEPS http://www.safetyandquality.gov.au/wp-content/uploads/2012/01/ossie.pdf