Download
1 / 1
10 likes | 138 Views
T=2 sec. T=7 sec. T=18 sec. “Lung Assist Device for term and preterm newborns with respiratory failure- Artificial Placenta ” Manan 1 , N. Rochow 2 , W. Wu 3 , G. Fusch 2 ,S. Monkman 2 , PR. Selvaganapthy 3 , C. Fusch 1,2

E N D
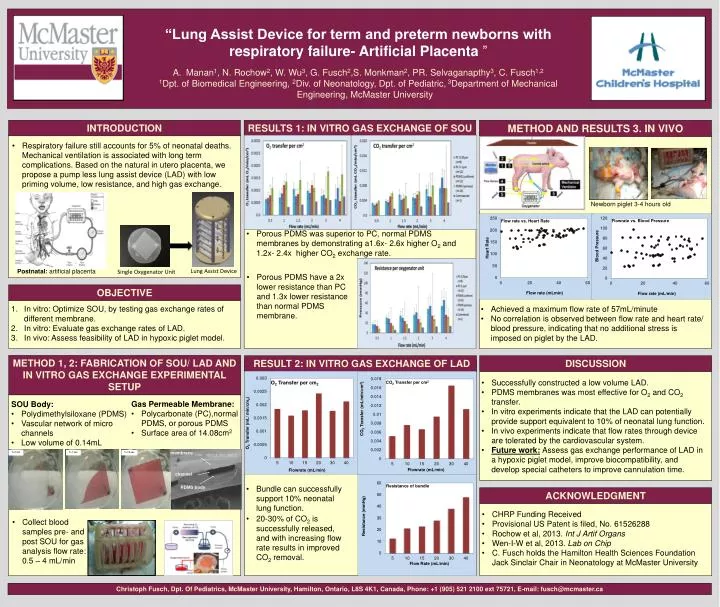
T=2 sec T=7 sec T=18 sec “Lung Assist Device for term and preterm newborns with respiratory failure- Artificial Placenta ” Manan1, N. Rochow2, W. Wu3, G. Fusch2,S. Monkman2, PR. Selvaganapthy3, C. Fusch1,2 1Dpt. of Biomedical Engineering, 2Div. of Neonatology, Dpt. of Pediatric, 3Department of Mechanical Engineering, McMaster University RESULTS 1: IN VITRO GAS EXCHANGE OF SOU METHOD AND RESULTS 3. IN VIVO INTRODUCTION • Respiratory failure still accounts for 5% of neonatal deaths. Mechanical ventilation is associated with long term complications. Based on the natural in utero placenta, we propose a pump less lung assist device (LAD) with low priming volume, low resistance, and high gas exchange. Newborn piglet 3-4 hours old • Porous PDMS was superior to PC, normal PDMS membranes by demonstrating a1.6x- 2.6x higher O2 and 1.2x- 2.4x higher CO2 exchange rate. Postnatal: artificial placenta Lung Assist Device Single Oxygenator Unit • Porous PDMS have a 2x lower resistance than PC and 1.3x lower resistance than normal PDMS membrane. OBJECTIVE In vitro: Optimize SOU, by testing gas exchange rates of different membrane. In vitro: Evaluate gas exchange rates of LAD. In vivo: Assess feasibility of LAD in hypoxic piglet model. • Achieved a maximum flow rate of 57mL/minute • No correlation is observed between flow rate and heart rate/ blood pressure, indicating that no additional stress is imposed on piglet by the LAD. membrane channel PDMS body METHOD 1, 2: FABRICATION OF SOU/ LAD AND IN VITRO GAS EXCHANGE EXPERIMENTAL SETUP DISCUSSION RESULT 2: IN VITRO GAS EXCHANGE OF LAD • Successfully constructed a low volume LAD. • PDMS membranes was most effective for O2 and CO2 transfer. • In vitro experiments indicate that the LAD can potentially provide support equivalent to 10% of neonatal lung function. • In vivo experiments indicate that flow rates through device are tolerated by the cardiovascular system. • Future work:Assess gas exchange performance of LAD in a hypoxic piglet model, improve biocompatibility, and develop special catheters to improve cannulation time. • SOU Body: • Polydimethylsiloxane (PDMS) • Vascular network of micro channels • Low volume of 0.14mL • Gas Permeable Membrane: • Polycarbonate (PC),normal PDMS, or porous PDMS • Surface area of 14.08cm2 • Bundle can successfully support 10% neonatal lung function. • 20-30% of CO2 is successfully released, and with increasing flow rate results in improved CO2 removal. ACKNOWLEDGMENT • CHRP Funding Received • Provisional US Patent is filed, No. 61526288 • Rochowet al, 2013. Int J Artif Organs • Wen-I-W et al, 2013. Lab on Chip • C. Fusch holds the Hamilton Health Sciences Foundation Jack Sinclair Chair in Neonatology at McMaster University • Collect blood samples pre- and post SOU for gas analysis flow rate: 0.5 – 4 mL/min Christoph Fusch, Dpt. Of Pediatrics, McMaster University, Hamilton, Ontario, L8S 4K1, Canada, Phone: +1 (905) 521 2100 ext 75721, E-mail: fusch@mcmaster.ca