Download
1 / 50
500 likes | 514 Views
Explore the intricate processes of respiration, ventilation, and gas exchange. Learn about gas laws, pulmonary physiology, respiratory disorders, and the vital role of chemoreceptors in maintaining homeostasis.

E N D
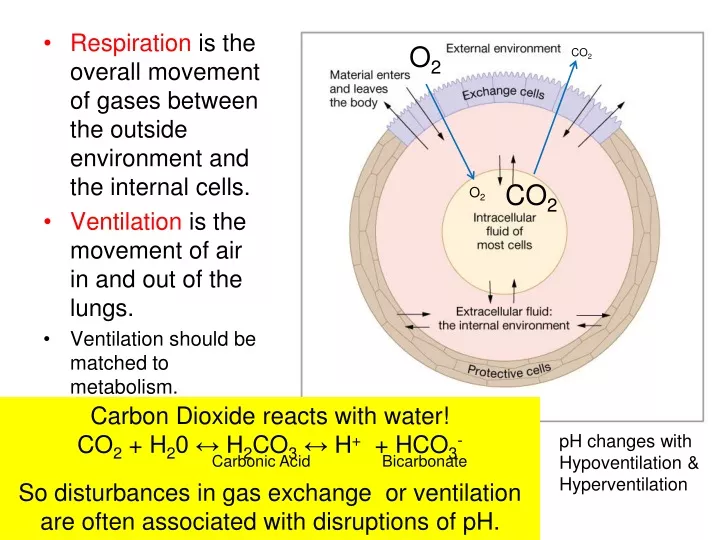
O2 CO2 • Respiration is the overall movement of gases between the outside environment and the internal cells. • Ventilation is the movement of air in and out of the lungs. • Ventilation should be matched to metabolism. CO2 O2 Carbon Dioxide reacts with water! CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- Carbonic Acid Bicarbonate So disturbances in gas exchange or ventilation are often associated with disruptions of pH. pH changes with Hypoventilation & Hyperventilation
Gas Laws Dalton’s Law Henry’s Law Gases dissolve in liquids in proportion to their partial pressure in the air in contact with that liquid • Total pressure = sum of partial pressures • PATM = P N2 + P O2 + P CO2 • 100% = 79% + 21% + <1% • P O2 = 0.21 x 760mmHg = 160 • Partial pressure of Oxygen in atmosphere at sea level is 160 mmHg • Regardless of elevation, air is always 21% O2. • N2 is physiologically inert; ignore except for decompression sickness air P O2 =160 mmHg liquid P O2 =160 mmHg
Why the difference in partial pressures in Air and Alveoli? Ventilation by Bulk Flow Gas exchange by Diffusion Where should the receptors be for the negative feedback loop for homeostasis? Gas exchange Gradient for CO2 is only 6 mmHg; CO2 is more soluble and permeable than O2
Gas exchange • All gases move by diffusion. Thus limited by: • Surface area • Distance • Concentration (partial pressure) gradient • In the lung, gases must move from air to water and vice versa. The amount is proportional to • Solubility (CO2 more soluble than O2) • Temperature (colder fluids dissolve more gas) • Pressure gradient
RespiratoryPhysiology The physics of air flow Flow in tubes 2) Ventilation Poiseulle’s equation
The Structure underlying the function: Upper Respiratory Tract Lower Respiratory Tract Intercostal muscles Bronchitis= infection/inflammation of conducting airways Asthma = smooth muscles contract →increase resistance to airflow in conducting airways.
Pneumothorax (unilateral due to each lung having its own compartment. Visceral pleura and parietal pleura separated by fluid-filled pleural cavity which allows lung and chest wall to slide relative to each other but remain adhered unless air enters the pleural cavity (which leads to collapse of the lung and outward expansion of chest wall on that side.) Greg R. and the story of spontaneous pneumothorax
Upper Tract Sleep Apneaa)obstructive,b)central & CPAP
RespiratoryEpitheliumof Airway(Not alveolus!) Mucus escalator Smoker’s hack
What does a river delta and your lungs have in common? Mixing of Freshwater (inspired air) and Salt water (alveolar air) Slower velocity of flow in delta (respiratory airways)
Figure 13-2 Particle Filtration: deposition varies Impaction Anatomical Dead Space Sedimentation Decrease In Flow Rate Brownian Diffusion
Pulmonary arterial blood = low in O2 Cartilage prevents collapse of airways during expiration. V/Q inequality = imperfect match between air flow and blood flow Response of pulmonary arterioles to low P O2
Matching blood flow (Q, also called “perfusion” ) to ventilation (V) by pulmonary arterioles that constrict in response to low O2anddilate in response to hi O2 (Note this response to O2 is opposite that of systemic arterioles!) Thus, poorly ventilated regions of the lung will receive less blood flow. So…. Q is “matched” to V, but not perfectly. And low perfusion in a region leads to bronchoconstriction.
Figure 22.10 5 liters of blood inpulmonary capillarieswith surface area equal to a tennis court
Type I pneumocytes are simple squamous epithelia that comprise the majority of the surface area. Type II pneumocytes secrete surfactant. Gas exchange by diffusion based on gradients.
Figure 13.17 Who cares? Respiratory Distress Syndrome of the Newborn Law of LaPlace Surfactant reduces surface tension which reduces the mechanical effort of ventilation and prevents the collapse of smaller alveoli.
Figure 13.19 Tidal inspiration At end of normal tidal expiration
V = VT x f VA = (VT – VDS) x f Anatomic dead space = air remaining in conducting zone (typically 150 ml.) What is VA if Tidal Volume is 150 ml?
O2 uptake CO2 production
CO2 production = Respiratory Quotient O2 uptake =0.8 for mixed diet 200mlCO2/min250 ml O2/min = 0.8 for proteins = 0.7 for fat = 1.0 for carbohydrate C6H12O6 + 6 O2 → 6 CO2 + 6 H2O + energy
Where are receptors for negative feedback loop? Gas exchange
Peripheral Chemoreceptors • Carotid bodies (not carotid sinuseswhich are baroreceptors) • Aortic bodies (not aortic arch baroreceptors) Central Chemoreceptors in medulla (sensitive to H+ in interstitial fluid of medulla) To ponder: Why should there be three sets of chemoreceptors?
Carbon Dioxide reacts with water! CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- Carbonic Acid Bicarbonate H+ can’t cross Blood Brain Barrier but CO2 does! Central Chemoreceptors respond to H+ produced bydiffusion of CO2 into brain interstitial fluid.
In what forms are O2 and CO2 found in the blood? Gas exchange
Figure 13.27 Partial Pressures are the same, but total oxygen content differs! Bound & Free CO2 andO2 bound to Hb do not contribute to partial pressure (no longer a dissolved gas!) Peripherial chemoreceptors can detect ONLY dissolved gasses!
Figure 13.31 Hb can bind O2, CO2, and H+ 100 40 100 Increases in CO2 and H+ decrease the affinity of Hb for O2
Steep Flat
Shifting the Oxyhemoglobin dissociation curve At 40 Torr, more DPG, higher temperature, and greater acidity (all indicative of increased metabolism) shift dissociation curve down (Hb has a lower affinity for O2) and thus more O2 is unloaded into the tissues. Notice the main affect is on the steep portion of the curve which means that there is little influence on the loading of O2 onto Hb in the lungs
Figure 13.34 Ventilation is relatively unaffected by PaO2 until it falls below 60. Explain why!
carbaminohemoglobin Chloride Shift CA = carbonic anhydrase Hb is a Buffer Carbon dioxide transport
40 46 carbaminohemoglobin 40 46
Any deviation from the set point for CO2 Causes immediate changes in ventilation! Why should this be so?
CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3- Carbonic Acid Bicarbonate
Figure 13.22 S 3
S 4 Figure 13.32 Negative feedback loop for control of blood gases Cervicalspinal cordinjury
Figure 13.40 S 5 Name the components of the negative feedback loop
S 6 Respiratory Physiology during Exercise Blood gases and pH change very little except when exercise is intense. Therefore, changes in minute ventilation are not the result of negative feeback. How can this be?
S 7 Negative feedback operates! But the changes in ventilation at the onset and offset of exercise cannot be explained by negative feedback. Experience, learning, modification of motor program, feed forward!
Figure 13.43 S 8 Integrator