Download
1 / 24
340 likes | 1.04k Views
Spinal Cord Injury. Kirsten Natasha Lindsey Vickie Laura. General Overview. Spinal Cord Injury is damage to the spinal cord that results in a loss of function such as mobility or feeling. Frequent causes of damage are trauma and disease.

E N D
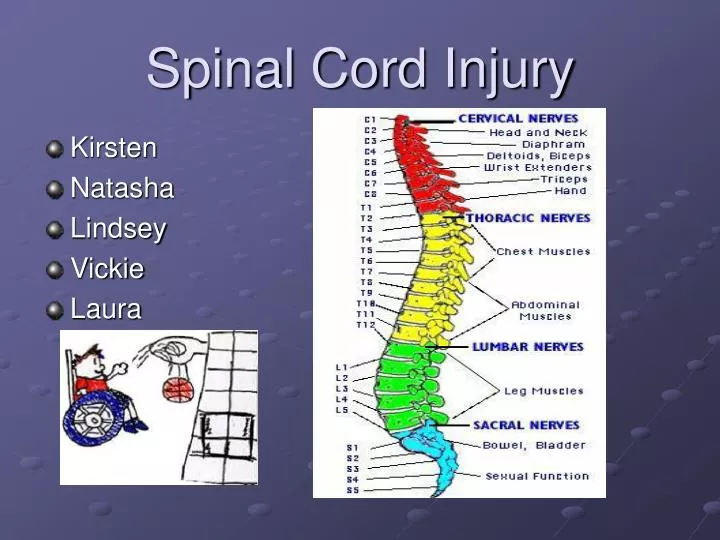
Spinal Cord Injury • Kirsten • Natasha • Lindsey • Vickie • Laura
General Overview • Spinal Cord Injury is damage to the spinal cord that results in a loss of function such as mobility or feeling. Frequent causes of damage are trauma and disease. • Spinal Cord is the major bundle of nerves that carry impulses to/from the brain to the rest of the body. • Spinal Cord is surrounded by rings of bone-vertebra. They function to protect the spinal cord.
Prognosis • Patients with a complete cord injury have a less than 5% chance of recovery. If complete paralysis persists at 72 hours after injury, recovery is essentially zero. • The prognosis is much better for the incomplete cord syndromes. • If some sensory function is preserved, the chance that the patient will eventually be able walk is greater than 50%. • Ultimately, 90% of patients with SCI return to their homes and regain independence. • In the early 1900s, the mortality rate 1 year after injury in patients with complete lesions approached 100%. Much of the improvement since then can be attributed to the introduction of antibiotics to treat pneumonia and urinary tract infection. • Currently, the 5-year survival rate for patients with a traumatic quadriplegia exceeds 90%. The hospital mortality rate for isolated acute SCI is low.
Scale of Motor Strength in SCI • The American Spinal Injury Association: • 0 - No contraction or movement • 1 - Minimal movement • 2 - Active movement, but not against gravity • 3 - Active movement against gravity • 4 - Active movement against resistance • 5 - Active movement against full resistance • Assessment of sensory function helps to identify the different pathways for light touch, proprioception, vibration, and pain. Use a pinprick to evaluate pain sensation.
Types of Spinal Cord Paralysis • Depending on the location and the extent of the injury different forms of paralysis can occur. • Monoplegia- paralysis of one limb • Diplegia- paralysis of both upper or lower limbs • Paraplegia- paralysis of both lower limbs • Hemiplegia- paralysis of upper limb, torso and lower leg on one side of the body • Quadraplegia- paralysis of all four limbs
Spinal Cord Paralysis Levels C1-C3 • All daily functions must be totally assisted • Breathing is dependant on a ventilator • Motorised wheelchair controlled by sip and puff or chin movements is required C4 • Same as C1-C3 except breathing can be done without a ventilator C5 • Good head, neck, shoulder movements, as well as elbow flexion • Electric wheelchair, or manual for short distances C6 • Wrist extension movements are good • Assistance needed for dressing, and transitions from bed to chair and car may also need assistance C7-C8 • All hand movements • Ability to dress, eat, drive, do transfers, and do upper body washes
Spinal Cord Paralysis Levels T1-T4 (paraplegia) • Normal communication skills • Help may only be needed for heavy household work or loading wheelchair into car T5-T9 • Manual wheelchair for everyday living • Independent for personal care T10-L1 • Partial paralysis of lower body L2-S5 • Some knee, hip and foot movements with possible slow difficult walking with assistance or aids • Only heavy home maintenance and hard cleaning will need assistance
Complete and Incomplete Spinal Cord Syndromes can be classified into either complete or incomplete categories • Complete – characterized as complete loss of motor and sensory function below the level of the traumatic lesion • Incomplete – characterized by variable neurological findings with partial loss of sensory and/or motor function below the lesion
Spinal Shock • An immediate loss of reflex function, called areflexia, below the level of injury • Signs: • Slow heart rate • Low blood pressure • Flaccid paralysis of skeletal muscles • Loss of somatic sensations • Urinary bladder dysfunction • Spinal shock may begin within an hour after injury and last from several minutes to several months, after which reflex activity gradually returns
Central Cord Syndrome • Usually involves a cervical lesion • May result from cervical hyperextension causing ischemic injury to the central part of the cord • Motor weakness is more present in the upper limbs then the lower limbs • Patient is more likely to lose pain and temperature sensation than proprioception • Patient may complain of a burning feeling in the upper limbs • More commonly seen in older patients with cervical arthritis or narrowing of the spinal cord
Brown-Sequard Syndrome • Results from an injury to only half of the spinal cord and is most noticed in the cervical region • Often caused by spinal cord tumours, trauma, or inflammation • Motor loss is evident on the same side as the injury to the spinal cord • Sensory loss is evident on the opposite side of the injury location (pain and temperature loss) • Bowel and bladder functions are usually normal • Person is normally able to walk although some bracing or stability devices may be required
Anterior Spinal Cord Syndrome • Usually results from compression of the artery that runs along the front of the spinal cord • Compression of SC may be from bone fragments or a large disc herniation • Patients with anterior spinal cord syndrome have a variable amount of motor function below the level of injury • Sensation to pain and temperature are lost while sensitivity to vibration and proprioception are preserved
Pre-hospital Care • Most pre-hospital care providers recognize the need to stabilize and immobilize the spine on the basis of mechanism of injury, pain in the vertebral column or neurological symptoms. • Patients are usually transported to the hospital with a cervical hard collar on a hard backboard. • Commercial devices are available to secure the patient to the board. • The patient should be secured so that in the event of vomiting, the backboard may be rapidly rotated 90 degrees while the patient remains fully immobilized in neutral position. Spinal immobilization protocols should be standard in all pre-hospital care systems.
Kinesiologist’s Role • Perform Subjective and Objective Assessment • Analyse the situation and determine your diagnosis • Plan how you will treat the condition. Includes consultation with or referral to other areas of the medical community
What can a Kinesiologist Do • Evaluate a person's ability and level of functioning in his or her home, at work, and while engaging in leisure activities and hobbies. • Determine how motivated a person is to participate in activities that he or she participated in prior to the injury. • Identify any changes in roles a person may experience as a result of SCI. • Provide individualized therapy to retrain people to perform daily living skills using adaptive techniques. • Facilitate coping skills that could help a person overcome the effects of SCI. • Implement exercises and routines that strengthen muscles that may have been affected that are necessary in daily activities, such as dressing, eating, and taking care of a home. • Determine the type of assistive devices that could help a person become more independent with daily living skills.
Basic Life Changes • The Kinesiologist will need to determine through conversation with the client, as well as subjective and objective assessment: • Eating • Dressing • Bowel/Bladder function • Weight Management- nutrition and fitness • Respiratory Issues • Pain • Psychosocial Issues • Sex and Pregnancy • Independence
Equipment / Accessibility • Kinesiologist should plan with client ways to improve personal mobility: • Homes • Vehicles • Public Access • Types of wheelchairs, mobility devices, splinting and seating available
Psychosocial Issues • These topics should be covered with the client, but will most likely be referred to another professional for: • Aging • Education/Employment • Family/Relationships • Psychosocial Adjustments • Rehabilitation • Sex • Substance Abuse
Treatment Fields • Occupational Therapy • Physiotherapy • Physicians • Social Workers • Therapeutic Recreation • Rehabilitation • Psychologists • Vocational Counsellors • Nutrition Assistance • Telemedicine-employing a SCI caregiver
Neurosurgery Neurology Urology Orthopedics Plastic Surgery Neuropsychology Internal Medicine Gynecology Driver Education Rehabilitation Engineering Chaplaincy Pulmonary Medicine General Surgery Psychiatry Speech Pathology Partners to Consult
Treatment Focus • The treatment team must specialize in treating SCI • The focus should be on family and patient participation where the clients personal abilities are maximized towards independence • Client should be a principal contributor to treatment decisions and goal making • Treatment should be on a regular scheduled basis for at least three hours per day
Questions • Can a person break their back/neck, but not sustain a spinal cord injury? A) Yes B) No C) Maybe D) Only in a MVA • Christopher Reeve used a what to get around? A) Suck and blow B) Ski’s C) Sip and Puff D) Wagon • What are 4 types of Paralysis? A) hemiplegia, diplegia, quadraplegia, paraplegia B) hemiplegia, hyperplegia, biplegia, triplegia C) hemiplegia, tetraplegia, homoplegia, heteroplegia D) hemiplegia, preplegia, sensiplegia, motorplegia
References • http://www.spinalinjury.net/html/_spinal_cord_101.html • http://www.spinalcord.org/ • http://www.spinalcord.uab.edu/show.asp?durki=19679 • http://www.wheelessonline.com/ortho/central_cord_syndrome_1 • http://www.ninds.nih.gov/disorders/central_cord/central_cord.htm • http://orthoinfo.assos.org/fact//thr_report.cfm?THread_ID=285&topcategory=Spine • http://www.emedicine.com/orthoped/topic39.htm • http://www.emedicine.com/emerg/topic70.htm • http://www.emedicinehealth.com/Articles/64223-1.asp • http://www.neuro.wustl.edu/sci/physiolo.htm#Central%20Cord%20Syndrome • http://www.emedicine.com/emerg/topic553.htm • http://www.apparelyzed.com/paralysis.html • http://www.spinalcord.uab.edu/show.asp?durki=22408 • http://www.spinalcord.org/html/newinjury/basic.php • http://images.main.uab.edu/spinalcord/html/Spas_Hy_files/frame.htm • http://www.spinalcord.org/html/injury.php • http://www.spinalinjury.net/index.html • http://www.spinalcord.uab.edu/ • http://canparaplegic.org/national/level2.tpl?var1=story&var2=20001027122552






















