Download
1 / 49
630 likes | 1.72k Views
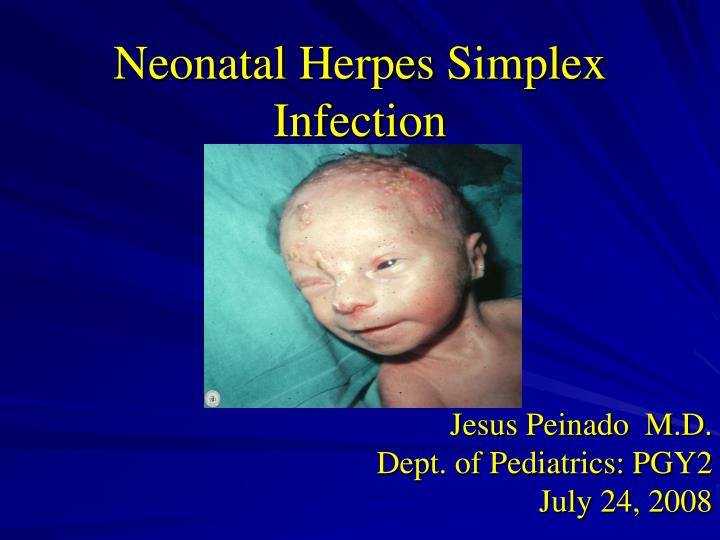
Neonatal Herpes Simplex Infection. Jesus Peinado M.D. Dept. of Pediatrics: PGY2 July 24, 2008. INTRODUCTION. Neonatal HSV infections were first described in the mid-1930s. The earliest antiviral agents proved too toxic in humans to be useful.

E N D
Neonatal Herpes Simplex Infection Jesus Peinado M.D. Dept. of Pediatrics: PGY2 July 24, 2008
INTRODUCTION • Neonatal HSV infections were first described in the mid-1930s. • The earliest antiviral agents proved too toxic in humans to be useful. • Vidarabine was the first systemically administered antiviral medication.
VIRAL STRUCTURE • Large and enveloped virions • Icosahedral nucleocapsid consisting of 162 capsomeres • Arranged around a linear, double stranded DNA core • The genome consists of 2 covalently linked components
VIRAL STRUCTURE Core: Consists of a single linear molecule of dsDNa in the form of a torus Capsid: Surrounding the core w/ a 100 nm diameter and 162 capsomeres Tegument: Consists of viral enzymes Envelope: Outer layer composed of altered host membrane and a dozen of viral glycoproteins
VIRAL STRUCTURE • There is considerable cross-reactivity between HSV-1 and HSV-2 glycoproteins • Unique antigenic determinants exist for each virus • Eleven glycoproteins have been identified • They mediate attachment, penetration and provoke immune responses
VIRAL STRUCTURE • gD is the most potent inducer in neutralizing antibodies • gD is related to viral entry into the cell • gB is related to infectivity • gG provides w/ antigenic specificity w/ the resulting antibody response allowing distinction between HSV-1 and HSV-2
BIOLOGY • Latency and neurovirulence directly influence on human disease • During HSV infection , virions are transported by by retrograde flow along axons • Vioral multiplication occurs in a small number of sensory neurons • Viral genome remains in a latent state for the life of the host
BIOLOGY • Periodic reactivation brought on by events of physical or emotional stress • The virus is transported back down the axon to replicate again at or near the point of entry • Reactivation can result in apparent disease (lesions) or clinically inaparent (subclinical) infection • Latency is incompletely understood
BIOLOGY • Neurovirulence is the affinity with which HSV is drawn to and propagated in neuronal tissue • This can result in profound disease with severe neurologic sequela • Sites for neuurovirulence have been mapped to the thymidine kinase gene • The gene identified as Y134.5 is required for replication in the CNS and prevents apoptosis of infected cells
MATERNAL GENITAL INFECTIONS • Most common form of genital infection during gestation • 10% of HSV-2 seronegative pregnant women have an HSV-2 seropositive partner • 2/3 of women who acquire genital herpes during pregnancy have no symptoms • 60 to 80% of women who deliver an HSV-infected infant have no evidence of infection
NEONATAL TRANSMISSION • Gravid woman must be shedding virus w/ or w/out symptoms • In non-pregnant HSV-seropositive women HSV as detected by PCR is shed w/out symptoms 1 of every 3 days • Among pregnant women the viral excretion proximate to delivery from 0.20 to 0.39% • Pregnant women w/ recurrent genital HSV the incidence is from 0.70 to 1.4%
FACTORS INFLUENCING TRANSMISSION • Type of maternal infection (primary/recurrent) • Maternal antibody status • Duration of rupture of membranes • Integrity of mucocutaneous barriers • Mode of delivery (C-section/vaginal)
INCIDENCE OF NEONATAL DISEASE • 2/1000 mothers are HSV culture + at delivery asymptomatic • 50-70% affected infants born to women asymptomatic at the time of delivery • Antepartum cultures are not useful in assessing risk of neonatal infection • Increased risk w/ primary vs recurrent infection • Incidence from 1/2000 to 1/5000 live births and increasing
RISK OF NEONATAL HSV INFECTION • 50% risk: Infants born to women w/ primary infection near the time of delivery • 30% risk: Infants born to mothers with first episode, non-primary infection (antibody to type 1, new acquisition type 2 and vice versa) • 1 to 3% of infants born to mothers w/ recurrent infection • Passive immunity protects against infection , but has little effect on the severity of disease
RISK FACTORS • Associated w/ primary maternal HSV: • Genital symptoms, UTI symptoms not responsive to therapy • Positive HSV cultures from both cervix and vagina • New sexual partner immediately prior to or during pregnancy
RISK FACTORS • Reasons for increased risk w/ primary maternal HSV infection • Prolonged shedding of virus up to 3 wk vs 2 to 5 days • Increased number of viral particles excreted • Less passive immunity to HSV, i.e. less maternal-fetal transfer of HSV neutralizing antibodies
RISK FACTORS • Neonatal risk factors: • Rupture of membranes > 6 hrs • Scalp electrodes or other internal monitoring • Chorioamnionitis • Cervicitis • Vaginal delivery
TIMES OF TRANSMISSION • HSV of the newborn is acquired during one of three distinct time intervals: • Intrauterine (in utero 5%) • Peripartum (perinatal 85%) • Psotpartum (postnatal 10%)
DISEASE CLASSIFICATION • Disease localized to the skin, eyes and mouth SEM disease accounting for 45% of cases • Encephalitis w/ or w/out CNS involvement accounting for 30% • Disseminated infection including CNC, lungs, etc. accounting for 25% • This classification is predictive of morbidity and mortality
INTRAUTERINE INFECTION • Occurs in 1/300,000 deliveries • Cutaneous manifestations: scarring, active lesions, hypo and hyperpigmentation, aplasia cutis and an erythematous macular exanthem • Ophthalmologic: microopthalmia, retinal dysplasia, optic atrophy, chorioretinitis • Neurologic: microcephaly, encephalomalacia, hydranencephaly, intracranial calcification
DISSEMINATED DISEASE • 1/2 to 2/3 of all children w/ neonatal HSV • Encephalitis is a common component occurring in about 60% to 75% • 20% w/ disseminated disease do not develop vesicular rash • Death relate to severe coagulopathy, liver dysfunction and pulmonary involvement
CNS DISEASE • 1/3 of all neonates w/ HSV infection w/ or w/out SEM involvement • Manifestations include: seizures (focal and generalized), lethargy, irritability, tremors, poor feeding and bulging fontanelle • 60 to 70% have associated skin vesicles • Mortality is cause by brain destruction w/ acute neurologic and autonomic dysfunction
LABORATORY ASSESSMENT • Type-specific antibody assays have been approved by FDA • Serologic testing identifies only past infection • Can not identify the site of HSV infection • Serological diagnosis is not of clinical value • Transplacentally acquired IGg confounds the assessment of neonatal antibody status • Serologic studies play no role in diagnosis
VIRAL CULTURE • Remains the definitive diagnostic method • If skin lesions scraping of the vesicles • Other sites include: CSF, urine, blood, stool or rectum, oropharynx and conjunctiva • Duodenal aspirates if hepatitis/NEC/GI disease • Of the sites cultured for HSV skin, eye and conjunctiva provides the greatest yields
PCR AMPLIFICATION PCR results from CSF of infected neonates No. (%) of patients with: • PCR result SEM (n29) CNS (n34) Disseminated (n14) • Positive 7 (24) 26 (76) 13 (93) • Negative 22 (76) 8 (24) 1 (7)
TREATMENT & MANAGEMENT • Mortality in preantiviral era by 1 y of age was 85% disseminated and 50% CNS disease • W/ high dose acyclovir 60mg/kg/day 12mo mortality for disseminated 29% and 4% for CNS disease • Lethargy/hepatitis are associated w/ mortality in disseminated disease • Prematurity/seizures in CNS disease
TREATMENT • Topical agents (trifluridine) are recommended for use along w/ parenteral acyclovir for ocular disease • IVIG has no value in the treatment of HSV • Higher doses of acyclovir are associated w/ neutropenia • Adequate hydration reduces risk of nephrotoxicity
SUMMARY OF CURRENT TREATMENT • Acyclovir 60mg/kg/day improves morbidity and mortality • In preterm dosing interval based on CrCl • Disseminated and CNS disease 21 days • SEM 14 days • All patients w/ CNS disease should have a repeat LP at the end of therapy • CSF w/ + PCR should continue treatment until PCR negative
PCR results following completion of antiviral therapy No. (%) with PCR result Infant characteristic Negative Positive P • Disease classification CNS disease 4 (36.4) 14 (73.7) < 0.001 Disseminated disease 0 (0.0) 5 (26.3) SEM disease 7 (63.6) 0 (0.0) • CSF indices Normal 6 (54.5) 1 (5.3) Abnormal 3 (27.3) 17 (89.4) • Morbidity/mortality >12 mo Normal 6 (54.5) 1 (5.3) <0.001 Mild 0 (0.0) 0 (0.0) Moderate 1 (9.1) 3 (15.8) Severe 2 (18.2) 10 (52.6) Dead 0 (0.0) 5 (26.3) Unknown 2 (18.2) 0 (0.0)
ANTIBODY THERAPY • Utilization of passive immunotherapy as adjuvant to active antiviral interventions • Human and humanized monoclonal Ab against gB or gD are benefical in animal models • Studies w/ humans have documented protective effects
VACCINE DEVELOPMENT • HSV-2 gD adjuvanted w/ alum combined w/ 3-deacylated monmophosphoryl lipid A has demostrated promising results • 75% efficacy in preventing HSV-1 HSV-2 genital disease • 40% efficacy in preventing HSV-2 infection
RECOMMENDATIONS • Pregnant women w/ primary or first episode: Acyclovir therapy at 36 wk 400mg tid • Primary HSV in 3rd trimester: C-section should be offered where lesions can occur within 6 wk of anticipated delivery and seroconversion has not occurred yet • Recurrent HSV: Acyclovir at 36 wk 400 mg tid
RECOMMENDATIONS • Women in labor: HSV lesions C-section may reduce the risk if performed 4-6 hrs ROM • Many recommend C-section even if ROM >6 hrs • If term and active lesions C-section • If preterm Acyclovir 15mg/kg/day • If no lesions only history VD • If genital lesions No invasive procedures (scalp sampling or monitors or early ROM)
INFANTS BORN BY NSVD CULTURES • Asymptomatic infants exposed to HSV • Mother had HSV but no lesions at delivery • Should be taken from urine, stool, rectum, mouth, eyes and nasopharynx • If therapy is initiated a CSF sample should be obtained prior to treatment • Duration of therapy is 14 to 21 days
INFANTS BORN BY NSVD • Acyclovir therapy is not recommended for the asymptomatic infant • Symptomatic infants PCR testing of CSF and blood • The index of suspicion should be maintained for 6 wk • HSV infection may occur as late as 4-6 wk after delivery
INFECTION CONTROL MESASURES • Contact precautions • Hand washing before and after care of infants • Mother w/ lesions on hands hand hygiene and gloves • BF is allowed if no lesions on the breast and if active lesions are covered • Mother w/ herpes labialis or stomatitis should wear disposable masks
DIAGNOSTIC TESTS • Cultures from skin lesions, mouth, nasopharynx, conjunctiva, urine, stool/ano-rectum and CSF. • Positive cultures at more than 48 hrs are consistent w/ viral replication as opposed to colonization • Serologic tests should not be relied on • PCR testing for CSF HSV DNA is the diagnostic method of choice for HSV encephalitis
TREATMENT AND FOLLOW UP • Acyclovir is the treatment of choice • SEM 14 days of treatments • CNS and disseminated disease 21 days • Oral acyclovir contraindicated in neonates for HSV treatment • Ocular involvement requires trifluridine
FUTURE RESEARCH ISSUES • The optimal management of pregnant women w/ genital HSV as this relates to antenatal acyclovir • The management of women w/ known or primary HSV who present w/ PROM • The pharmacokinetics of acyclovir in VLBW • The significance of acyclovir-resistant HSV from neonates w/ prolonged exposure
FUTURE RESEARCH ISSUES • The role of new agents such as famciclovir and valacyclovir where oral therapy is desired • The impact of long-term suppressive therapy on neurological outcomes and immune responses • Development/standardization of PCR on different body fluids • Role of combination antiviral therapy w/ acyclovir plus monoclonal HSV antibodies • Development of vaccines against HSV
REFERENCES • Neonatal Herpes Simplex Infection, Kimberlin David; Clinical Microbiology reviews, Jan 2004 p 1-13. • AAP 2005, Herpes Simplex, p 309-318. In L.K. Pickering (ed.) 2005 Red Book. • Current management of HSV infection in pregnant women and their newborn infants, Canadian Paediatric Society, Paediatrics and Child health 2006;11:363-5