Download
1 / 41
410 likes | 424 Views
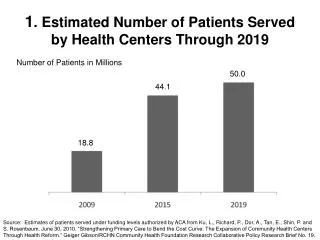
Decreasing the Number of Patients Sent to the Outpatient Diagnostic Centers with No Lab Orders. Presenters: Charisse Acosta, CT (ASCP), SSGB, CQIA and Joan Woods, MLT, SSGB Office of Quality Improvement, Pathology and Laboratory Medicine. 1.

E N D
Decreasing the Number of Patients Sent to the Outpatient Diagnostic Centers with No Lab Orders Presenters: Charisse Acosta, CT (ASCP), SSGB, CQIA and Joan Woods, MLT, SSGB Office of Quality Improvement, Pathology and Laboratory Medicine 1
Office of Quality Improvement,Pathology and Laboratory Medicine OUR MISSION: To support the Division of Pathology and Laboratory Medicine in consistently exceeding accreditation, safety, and regulatory compliance requirements and in driving sustainable improvement through the use of systematic quality methodologies.
Office of Quality Improvement,Pathology and Laboratory Medicine OUR GROUP: Team of 4 Quality Technologists – MLT, MT, CT, Lean Training, SSGG, Over 50 years combined laboratory experience Project Director – Industrial Engineer, SSBB, MBA PROJECTS: • Lab Layout Design • Workflow Improvement • Turnaround Time Reduction • Material Management • Waste Reduction
Background 2010 PI Project: Reduce Patient wait Time in the Outpatient Diagnostic Centers - Converted to a pull process - Moved patient sign-in away from front desk
Background Results: Goals: Decrease patient wait time Decrease congestion and confusion at front desk Increase patient satisfaction Increase on time arrival to downstream appointments
Background 2011 Phlebotomist 5S Project: Standardized workstations Organized Fully stocked Labeled
Background 2011 Diagnostic Center PSC Workflow Project:- Clarified patient sign-in form - Issues identified and categorized - Intradepartmental issues improved - Outside Issues prioritized
The Team Facilitator: Ron Phipps, PLM QI Project Director Champion: Bob Del Guidice, CAD, General Services Sponsor: Dr. Elizabeth Wagar, Chair, Laboratory Medicine • CS&E Team Members: Charisse Acosta, Joan Woods, Vijaya Bapat, Starnisha Anderson-Moore, Yvette Bobb and Lisa Thomas
Contributing Partners Diagnostic Centers: Ashley Williams (Clark Clinic), Luz Hurtado (Mays Clinic) Lymphoma Clinic: RaShaundra Jacobs, Cynthia Jenkins Anesthesia Assessment: Rosemary McCullar Holli Williams GI Clinic: Jessica Campbell Veronica Smith GYN Center: Russell Content Breast Center: Stephanie Staten GU Center: Hamid Refai
Aim Statement The purpose of this project was to decrease the amount of patients arriving at Clark and Mays Diagnostic Centers for blood collection with no orders for labs by 50% before Aug 31, 2011.
Strategic Alignment Patient Care Strategy 1.2 - We will increase the quality, safety and value of our clinical care. Strategy 1.5 - We will enhance productivity, access and efficiency by strengthening our infrastructure and support systems. Resources Strategy 7.1 - We will continuously improve our administrative infrastructure to support the efforts of our people in achieving our mission through health information technology and quality improvement education and research.
Data Collection Methods • Clark and Mays Diagnostic Center PSC’s log each patient with no orders on a log sheet • Date • MRN • Clinic • Time patient presented • Time problem corrected in system • Additional comments
Baseline Metrics • Baseline data collected: May 3, 2011 – June 17, 2011 • Metrics Analyzed: • Daily total errors • Counts by Clinic • Time to correct • Special connectors
Baseline Measures • Average errors per day: 11 • Average time to correct: 23 minutes • Weekly Waste: • 21 hours of additional patient wait time • 26.5 hours PSC rework
Clark Clinic Baseline Average: 10.6 patients per day
Clark Clinic Value Stream Map Patient arrives Patient called for blood draw
Pareto ChartClark Baseline (5/31/2011 – 6/17/2011 67% of issues arise from 3 clinics
Stratifying the Data Anesthesia Assessment Center • Assumptions: • Patients are sent directly to the lab directly following Anesthesia appointment • Ordering is still in process when patient arrives at the lab • Clinic Service Requisition (CSR) has not been given to PSC for entering before patient leaves clinic - But how do we know for sure?
Stratifying the Data Q: How long does it take to correct Anesthesia problems? • Average overall time to correct: 23 mins • Average time to correct Anesthesia problems: 11 mins • Clinic Proximity to Lab Conclusion: Time to enter an order > Time for patient to arrive in DC
Stratifying the Data Lymphoma • 60% of 24 hr urine errors come from the Lymphoma Center Ordering: • 24 hr urine not included in panel workup code • Same day patients must have separate appointment for next day to return with urine specimen
Major Issues Identified • Underutilized daily CARE reports • Clinics are unaware that no orders were placed • 24 hr urines not ordered separately • Patients bring in 24 hr urines that were not ordered • DC PSC’s don’t have correct clinic numbers • Patients are sent to lab before clinic PSC receives Clinic Service Requisition (CSR)
Diagnostic Center Implemented Improvements • Updated clinic contact lists • Physician/PSC Team lists • Direct Clinic PSC lines • PSC Training on Phone Directory usage • CARE Missing Labs Report • Allows correction before patient arrives
Clark Clinic Implemented Improvements Anesthesia Assessment Center • Lab Check Out Desk Patients orders completed before leaving clinic Lymphoma/Myeloma • Retrain PSC’s on 24 hr urine ordering procedures • Utilize missing labs CARE report • New terminology for patient schedules
Very Similar Wording Confusing Patient Schedule Wording for Lymphoma Patients Blood and Urine Blood collection only
New Schedule Wording BLOOD/24 HR URINE COLLECTION or BLOOD ONLY or 24 HR URINE COLLECTION ONLY Patient has clear understanding of the appointment’s testing expectations
Overall Improvement Clark Clinic RESULTS – Overall Improvement Clark Clinic 73%Overall Improvement
Lymphoma Clinic Improvements 89% Improvement
Anesthesia Assessment Center Improvements 92% Improvement
Benefits • Soft Savings: • Avoided Rework • - 20 hours per week of employee time • - $16,545 per year • Wait Time • - Avoided 836 hours of additional patient wait time per year
Additional Benefits • Improved utilization of resources • - Increased productivity • - More on time arrivals to downstream appointments • Improved patient satisfaction • shorter, less stressful day for patients • trust in system • Improved Institution image • smooth, coordinated efforts between departments • professional, competent atmosphere • The right testing at the right time
In Progress/Next Steps Current: • Continued data collection • Continued work with additional clinics to find improvements • Currently piloting online CSR’s Future: • Incorporate business needs of the lab in the requirements for new patient scheduling system upgrade • Corrections to CSR’s • Expand use of order sets, online CSR’s, and CARE system reports
Our Keys to Success • Always back up your story with data • Great resources are the people that do the work or are effected by the work • Persistence is key • Buy in is crucial • Don’t be afraid to ask • Change is rewarding!
“Every system is perfectly designed to get exactly the results it gets.” - Anonymous In other words, if you don’t like the results… Change The System!
Thank you!Any Questions? Charisse Acosta bcacosta@mdanderson.org Joan Woods jtwoods@mdanderson.org