Download
1 / 13
130 likes | 296 Views
PLANNED CARE SERVICES THE CURRENT POSITION Paul Bamber Divisional Manager Planned Care Services. 28/01/09. High Level of Staff Commitment Range Of Skills Available Within the Workforce Numerous Examples of Excellent Practice Opportunities to Develop Services (IAPT, ADHD)

E N D
PLANNED CARE SERVICESTHE CURRENT POSITIONPaul BamberDivisional ManagerPlanned Care Services 28/01/09
. High Level of Staff Commitment Range Of Skills Available Within the Workforce Numerous Examples of Excellent Practice Opportunities to Develop Services (IAPT, ADHD) Differing Operational Management and Clinical Leadership Models Inadequate Capacity And Performance Management Information And Supporting Systems
Variable - Access and Exit Criteria - Access Points and Pathways - Practice Standards/Compliance - Delivery Models (Generic/Sub-Specialist) - Partnership Arrangements Inconsistent Communication/Engagement Strategy Workforce Development Strategy Not Joined Up Until Recently - No Agreed Framework for the Delivery of Services and Payment By Results – Timescales Very Tight
Mixed Reviews About Services From Commissioners, Referrers and Service Users/Carers Outdated Service Level Agreements/Budgets No Jointly Agreed Outcome Measures Efficiency Targets to be Achieved Over the Next 4 Years At Risk of Losing Services Without Significant Needs Led Redesign/Remodelling
PLANNED CARE SERVICES NEXT STEPS
Revise Service Management and Clinical Leadership Arrangements Develop Single Management Model Model to Facilitate the Development of Specialist Functions and Flexible Use of Resources Need to Clarify and Strengthen Clinical Leadership and Operational Management Arrangements Increased Focus on Partnership Working to Balance Functional Model
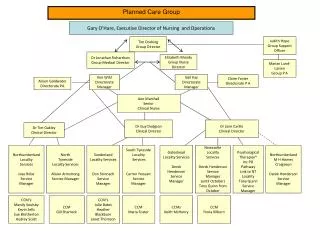
Clinical Leads for Each Team Divisional Manager Planned Care Services Associate Nursing Director/ Lead Nurses Associate/ Assistant Medical Directors AHP Leads Psych-therapy Leads Service Manager Service Manager LCM Urban North/land LCM G/head LCM Rural North/land LCM Ncle LCM Sunderland LCM S/Tyneside LCM N/Tyneside PCMHS Clinical Manager PCMHS Clinical Manager Develop Clinical Leadership Model Across Teams and Remove Team Manager Role
Improve Service Efficiency and Effectiveness Implement Capacity Management Framework Further Develop Performance Management and Clinical Leadership Skills Achievement of National and Local Practice Standards in Every Episode of Care Development of Performance and Quality Outcome Monitoring Framework Single Computerised Patient Records (RIO)
Implement Pathways and Packages Framework Roll Out Training Programme Clinical Engagement/Development Of Expert Users Establish Data Validation/Analysis Group Roll Out In Line With RIO Programme Cluster Analysis – Skill Mix/Capacity Requirements Pathways And Packages Development
Service Remodelling Single Point of Access and Development of Consistent Access/Exit Criteria Move From Generic CMHT to Sub Speciality Focus RTS Shared Care/Helpline IAPT Integration of Care Pathways/Service Strategies - Urgent Care/Rehabilitation - PD, DD, Psychological Therapy Strategies - Professional Groups
Workforce Planning/Development Confirm as is position Mandatory Training Requirements PDPs Linked to Service Development Priorities Skills Development – Pathways and Packages Implications of Service Redesign on the Workforce Review Roles in line with new ways of working Skills Register
Accommodation Sunderland Gateshead/South Tyneside Newcastle/North Tyneside Northumberland • Communication/Engagement Strategy • Users/Carers • Commissioners • Partner Agencies And Other Key Stakeholders
Re-establish Service Wide Steering Group Establish Divisional Sub Groups Agree Arrangements For Involvement With Stakeholders Draft Service Development Strategy Paper Service Wide High Level Action Plan Supported By Local Action Plans 8. Managing Service Remodelling/Redesign