Download
1 / 67
670 likes | 781 Views
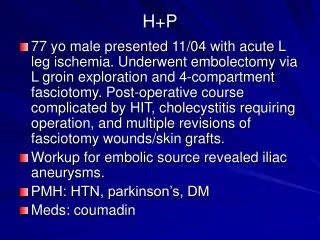
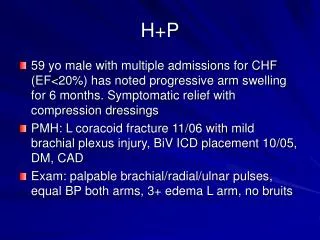
P aroxysmal N octurnal H emoglobinuria. New ideas about an old disease Ahmad Shihada Silmi Msc, FIBMS Staff Specialist in Hematology Medical Technology Department Islamic University of Gaza. Objectives. Try to answer some of the frequently asked questions about: The cause of the PNH

E N D
ParoxysmalNocturnalHemoglobinuria New ideas about an old disease Ahmad Shihada Silmi Msc, FIBMS Staff Specialist in Hematology Medical Technology Department Islamic University of Gaza
Objectives Try to answer some of the frequently asked questions about: The cause of the PNH The clinical presentation of PNH Diagnosing PNH The complications of PNH New treatments for PNH
What is PNH? • A disorder of blood affecting all the cells which come the bone marrow. • Prevalence 1-4 per million • The disease is quite rare, only 10, 000 patients in the US and Europe. • There is no ethnic preference for the disorder. • It may present early or late in life. • The manifestations may be “classic” or obscure.
PNH Prognosis • Significant morbidity and mortality • Patients have lived for extended periods of time and have seen spontaneous recovery • Report of 80 patients showed that 60% of deaths due to venous thrombosis or bleeding • Retrospective study of 220 patients • Kaplan-Meier survival 78, 65, and 48% at 5, 10, and 15 years • 8 year rates of major complications of PNH (pancytopenia, thrombosis, MDS) 15, 28, and 5% • Up to 5% of patients can develop acute leukemia; onset about 5 years after Dx of PNH • Likely incident of leukemia lower than 5%
What is PNH Mutation? • PNH is due to a mutation in a gene in a blood stem cell. • The gene is called the PIG-A gene (phosphatidylinositol glycan complementation group A) and is located on the X chromosome. • >100 mutations in PIG - A gene known in PNH • The mutations (mostly deletions or insertions) generally result in stop codons - yielding truncated proteins which may be non or partially functional - explains heterogeneity seen in PNH
What is PNH? • In most cases of PNH, the change in the gene (mutation) is acquired, not something you are born with. When and why is unknown. • The gene contains the genetic information for the GPI anchors which link proteins to the cell membrane
What is PNH? • A mutation is a “mistake” or a “change” in the gene that arises during copying and is not corrected • When the cell divides, the mutation is transmitted to daughter cells • The effect of a mutation: • None • An altered protein (sickle hemoglobin) • No protein is produced as in PNH, hemophilia etc
Stem Cells Egg Sperm Egg Embryonic Stem Cell Egg or Sperm Blood Muscle Nerve Etc. Somatic Stem Cells The Cells of Each Specific Organ
Stem Cells Egg Sperm Egg Embryonic Stem Cell Egg or Sperm Blood Muscle Nerve Etc. Somatic Stem Cells The Cells of Each Specific Organ
Stem Cells Egg Sperm Egg Embryonic Stem Cell Egg or Sperm Blood Muscle Nerve Etc. Somatic Stem Cells The Cells of Each Specific Organ
Stem Cells T LYMPHOCYTES STEM CELL B LYMPHOCYTES ERYTHROCYTES GRANULOCYTES MONOCYTES PLATELETS
Stem Cells T LYMPHOCYTES STEM CELL B LYMPHOCYTES ERYTHROCYTES GRANULOCYTES MONOCYTES ALTERED GENE PLATELETS
Stem Cells NORMAL CLONES ABNORMAL CLONE
N GPI-AP Biosynthesis:Involves 10 Steps and >20 Genes Plasma Membrane Raft N N PIG-A PI GlcNAc-PI Endoplasmic Reticulum
The Beginning of PNH The change that occurs in PNH stops the production of an anchor that ties protein molecules to the cell Sometimes the stop is only partial and PNH II cells occur
The GPI Anchor Defect in PNH PROTEIN Asp NORMAL C=O NH CH 2 CH 2 O O=P=O O ( 1-2) ( 1-6) ( 1-4) O O-P=O N O CH CH NH 2 2 2 O O-P-O O CH CH CH 2 2 C=O O O C=O (18:0,1) (16:0) (22:4,5) PNH O O-P-O O CH CH CH 2 2 O O C=O (18:0,1) (22:4,5)
Pathogenesis - The Defect GPI Anchor • PIG - A gene codes for 60 kDa protein glycosyltransferase which effects the first step in the synthesis of the glycolipid GPI anchor (glycosylphosphatidylinositol). Results in clones lacking GPI anchor - in turn, attached proteins PIG - A protein
What is PNH? • As a result of the PIG-A mutation, there is little of no GPI anchor produced. • PNH II cells- mild reduction • PNH III cells- severely reduced. • When the anchor is reduced, certain proteins can’t attach to the cells. • The most important proteins for PNH are CD 59, CD55.
Proteins anchored by GPI Anchorand Surface Proteins Missing on PNH Blood Cells Antigen Expression Pattern Enzymes Acetylcholinesterase (AchE) Red blood cells Ecto-5'-nucleotidase (CD73) Some B- and T-lymphocytes Neutrophil alkaline phosphatase(NAP) Neutrophils ADP-rybosyl transferase Some T-lymphs, Neutrophils Adhesion molecules Blast-I/CD48 Lymphocytes Lymphocyte function- associated antigen-3(LFA-3 or CD58) All blood cells CD66b Neutrophils Complement regulating surface proteins Decay accelerating factor (DAF or CD55) All blood cells Homologous restriction factor, Membrance inhibitor of reactive lysis All blood cells (MIRL or CD59)
Surface Proteins Missing on PNH Blood Cells Antigen Expression Pattern Receptors Fc- receptor III (Fc Rlll or CD16) Neutrophils, NK-cells, macrophages, some T-lymphocytes Monocyte differentiation antigen Monocytes, macrophages (CD14) Urokinase-type Plasminogen Monocytes, granulocytes Activator Receptor (u-PAR, CD87) Blood group antigens Comer antigens (DAF) Red blood cells Yt antigens (AchE) Red blood cells Holley Gregory antigen Red blood cells John Milton Hagen antigen (JMH) Red blood cells, lymphocytes Dombrock reside Red blood cells Neutrophil antigens NB1/NB2 Neutrophils
Surface Proteins Missing on PNH Blood Cells Antigen Expression Pattern Other surface proteins of unknown functions CAMPATH-1 antigen (CDw52) Lymphocytes, monocytes CD24 B-lymphocytes, Neutrophils, eosinophils p5O-80 Neutrophils GP500 Platelets GPI75 Platelets
PathogenesisCD 55 • Also known as decay accelerating factor • Accelerates decay of enzyme that destroys red cell membranes • CD55 inhibits the formation or destabilizes complement C3 convertase (C4bC2a) • When GPI anchor absent, CD55 not available and RBC membranes hemolyze
PathogenesisCD59 • Also known as membrane inhibitor of reactive lysis, protectin, homologous restriction factor, and membrane attack complex inhibitory factor • CD59 Protects the membrane from attack by the C5-C9 complex • Absence or reduction of CD59 leads to increased hemolysis and perhaps thrombosis
Pathogenesis of CD55 & CD59 • Inherited absences of both proteins in humans have been described • Most inherited deficiencies of CD55 - no distinct clinical hemolytic syndrome • Inherited absence of CD59 - produces a clinical disease similar to PNH with hemolysis and recurrent thrombotic events
Pathogenesis • Many normal people have very small numbers (perhaps 6 per 1,000,000 bone marrow cells) • In PNH, the abnormal cells have an advantage and become a major population in the marrow and blood (anywhere from 1% to over 90%) • This may be a result of change in the immune system –inability to recognize something foreign. • Or it may be related to aplastic anemia, a disease of poor production of blood from the marrow-WHY?
Pathogenesis - Clonal evolution and cellular selection • Expansion of abnormal hematopoietic stem cell required for PNH disease expression • Theories for expansion • Blood cells lacking GPI-linked proteins have intrinsic ability to grow abnormally fast • In vitro growth studies demonstrate that there are no differences in growth between normal progenitors and PNH phenotype progenitors • In vivo - mice deficient for PIG -A gene also demonstrates no growth advantage to repopulation of BM. • Additional environmental factors exert selective pressure in favor of expansion of GPI anchor deficient blood cells • Close association with AA - PNH hematopoitic cells cells may be more resistant to the Immune System than normal hematopoitic cells. • Evidence in AA is that the decrease in hematopoitic cells is due to increased apoptosis via cytotoxic T cells by direct cell contact or cytokines (escape via deficiency in GPI linked protein???)
PNH Clinical FeaturesAplastic Anemia • Some PNH patients have aplastic anemia or a history of aplastic anemia • Many PNH patients have evidence of a bone marrow that doesn’t work well or well enough to maintain normal blood counts • Therefore, whatever causes aplastic anemia (immune suppression or dysregulation or damage to the stem cells) may allow PNH to develop
What is PNH?Complement • Complement is a group of blood proteins that act together to help the body get rid of microbiological invaders • One of the ways it does this is by penetrating the membrane (outside surface) of the invading bacteria or viruses. • When this happens to PNH blood cells, the cells are destroyed.
What is PNH? Complement circulates in an inactive form • It is activated spontaneously and by a variety of events • It is normally activated more at night • It is more active with infections, trauma, vaccinations, surgery, immune complexes, autoimmune diseases
What is PNH?Complement • Complement activity is regulated by proteins in the blood and on the membranes of the cell. • Proteins on the cell surface interfere with complement to prevent breakdown (lysis) of the cell membrane • The most important of these is CD59, which is missing on the abnormal cells of PNH • For this reason, PNH red cells are extremely sensitive to very small amounts of activated complement
C5a C8 C6 C6 C6 C6 C6 C5 C7 CD59 C7 C7 C7 C7 CD59 C5b C5b C5b C5b C5b Absence of CD59 Allows Terminal Complement Complex Formation C9 C9 x 12 - 15 C8 X X C5 convertase C5 convertase Bb+ C3 C3b C9 C8 C8 C5b-9 C5b,6,7 C5b-8 Adapted from Cellular and Molecular Immunology AK Abbas, AH Litchman and JS Pober, 3rd Edition. 1991 WB Saunders; Philadelphia.
What is PNH? • Complement successfully attacks the red cells and they break up (hemolysis) • This releases hemoglobin (the red pigment in red cells) into the plasma • Causes anemia • Pieces of the membrane come off. • The white cells release granule contents and change to express other proteins. • The platelets form vesicles (membrane blisters) and activate.
P P What is PNH? Normal red blood cells are protected from complement attack by a shield of terminal complement inhibitors Without this protective complement inhibitor shield, PNH red blood cells are destroyed Complement activation
What is PNH?Clinical Features • Some of the hemoglobin passes through the kidneys and into the urine, causing red to dark brown urine (hemoglobinuria) • This causes a loss of iron from the body • In the long run, this may damage the kidney • Free hemoglobin binds nitric oxide causing vascular and smooth muscle spasm • Causes inflammation
Action of Nitric Oxide (NO) NO NO Smooth Muscle Relaxation Smooth Muscle Contraction
Free Hemoglobin Binds NO NO NO Smooth Muscle Relaxation NO Free Hemoglobin Smooth Muscle Contraction
What Are The Effects of Nitric Oxide Trapping by Hemoglobin Spasm of the esophagus Abdominal pain Erectile dysfunction Other symptoms such as “fatigue”
What is PNHClinical aspects • Vascular (arterial constriction, HBP) • Pulmonary artery pressure increase (PHTN) • Spasm of the esophagus • Abdominal pain • Erectile dysfunction • Other symptoms such as “fatigue” • Platelets are more “reactive”
What is PNH?Clinical Features • WBC: • Granulocytes - release content stimulating inflammation • Monocytes - activate expressing TF which leads to blood clots. TF-Microvesicles • Platelets become “activated” • They stick together and form clumps • The membrane changes, allowing them to bind to monocytes • Pieces of the membrane come off (microvesicles)
What is PNH?Clinical Features • Hemolytic anemia due to complement activation • Hemoglobinuria and, eventually, kidney damage • Anemia to a variable degree • Effects of NO depletion- HBP, smooth muscle dystonia, reduced blood flow to the kidney and lungs • Impaired bone marrow function
What is PNH?Clinical Features • Thrombosis (Blood clots) • Often in unusual places (liver veins, abdominal veins, cerebral veins, dermal veins) • Fatigue – overwhelming, poor correlation to level of hemoglobin • inflammation • anemia • Portal hypertension (PHTN).
Thrombosis in PNH Pathophysiology COMPLEMENT INJURY NO PS C5b-9 HEMOLYSIS MONOCYTES PLATELET Endothelial cells THROMBIN GENERATION COMPLEMENT C5a TF CYTOKINES IL-6 INFLAMMATION TF = Tissue factor.
Laboratory Evaluation of PNH • Acidified Serum Test (Ham Test 1939) • Acidified serum activates alternative complement pathway resulting in lysis of patient’s rbcs • May be positive in congenitial dyserythropoietic anemia • Still in use today • Sucrose Hemolysis Test (1970) • 10% sucrose provides low ionic strength which promotes complement binding resulting in lysis of patient’s rbcs • May be positive in megaloblastic anemia, autoimmune hemolytic anemia, others • Less specific than Ham test
Laboratory Evaluation of PNH • PNH Diagnosis by Flow Cytometry (1986) • Considered method of choice for diagnosis of PNH (1996) • Detects actual PNH clones lacking GPI anchored proteins • More sensitive and specific than Ham and sucrose hemolysis test
PNH Diagnosis by Flow Cytometry Of the long list of GPI anchored protein, monoclonal antibodies to the following antigens have been used in the diagnosis of PNH The most useful Abs are to CD14, 16, 55, 59, and 66. Are all required? Probably not - more studies needed AntigenCell LineageFunction CD14 monocytes LPS receptor, MDF CD16 neutrophils FcIII receptor CD24 neutrophils B-cell differentiation marker CD55 all lineages DAF CD58 all lineages possible adhesion CD59 all lineages MIRL, HRF, protectin CD66b neutrophils CEA-related glycoprotein
PNH Diagnosis by Flow Cytometry • Antigen expression is generally categorized into three antigen density groups • type I Normal Ag expression • type II Intermediate Ag expression • type III No Ag expression • Patient samples that demonstrate cell populations with diminished or absent GPI-linked proteins (Type II or III cells) with multiple antibodies are considered to be consistent with PNH. • Should examine multiple lineages (ie granulocytes & monocytes)
PNH Diagnosis by Flow Cytometry Examples of variable GPI linked CD59 expression on granulocytes on four PNH patients