Download
1 / 24
240 likes | 486 Views
Insomnia and poor sleep. Dr Phillippa Lawson Consultant sleep physician East Anglia. About me. Live in Saffron Walden Consultant in sleep, respiratory and general medicine at West Suffolk Hospital Founder of the good sleep programme Mother to two professors!. Outline. What is it?

E N D
Insomnia and poor sleep Dr Phillippa Lawson Consultant sleep physician East Anglia
About me • Live in Saffron Walden • Consultant in sleep, respiratory and general medicine at West Suffolk Hospital • Founder of the good sleep programme • Mother to two professors!
Outline • What is it? • Who does it affect? • How is it diagnosed? • What can be done?
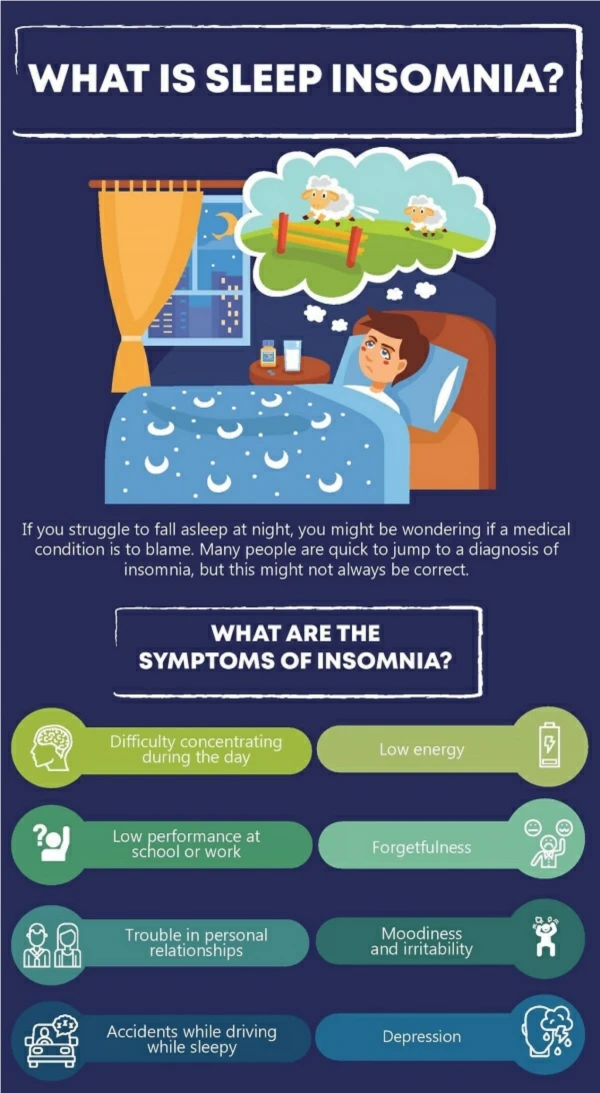
What is insomnia? • Difficulty falling asleep • Difficulty staying asleep • Early morning wakening • Non-refreshing or non-restorative sleep plus • Daytime symptoms • Prolonged
Who does it affect? • Anyone! • Prevalence 10 – 48 % depending on study methods • UK study§ found incidence to be 15 %, prevalence 37% • More common in females (55 %) • Median age 50 years (18 – 98) • Persistence of insomnia associated with increasing age • Associated with mental health problems • Associated with physical health problems • Associated with other sleep disorders §Morphyet al SLEEP 30 (3) 2007
What causes insomnia? • Precipitating factors • Acute stress • Illness (physical or mental) • Medications • Worry and rumination • Predisposing factors • Genetics • Hyperarousal • Depression • Tendency to worry and ruminate • Perpetuating factors • Dysfunctional attitudes about sleep • Staying awake in bed • Increased time in bed • Worry and rumination about insomnia
How do we diagnose it? • Who? Self-diagnose GP Specialist in sleep medicine • How? ‘Sleep history’ Questionnaires Sleep diary Actigraphy Polysomnogram
How do we diagnose it? • Who? Self-diagnose GP Specialist in sleep medicine • How? ‘Sleep history’ Questionnaires Sleep diary Actigraphy Polysomnogram
What can be done? Set your goals General wellbeing • Nutrition and fluid intake • Alcohol intake • Caffeine intake • Nicotine • Exercise • Sun light • Incorporating rest times • Positive attitude
What can be done? Preparing the sleep environment • Temperature • Bed and bedding • Light • Calm, uncluttered environment • Clocks and technology! ‘Sleep hygiene’ • Regular bed/rise times • Avoiding napping • ‘Wind down’ routine
What can be done? Stimulus control • Get out of bed when can’t sleep • Stop all sleep-incompatible activities • Strengthen the bed-sleep association Sleep restriction • Reduce time in bed to actual sleep time • Shorten time in bed • Improves sleep efficiency and strengthens bed-sleep association • Avoids disrupted and fragmented sleep
Sleep efficiency Total sleep time (time from falling asleep to time you woke for final time minus estimated time spent awake during night) ÷ Total time in bed (time from lights out to time you finally got up) X 100
What can be done? Stimulus control • Get out of bed when can’t sleep • Stop all sleep-incompatible activities • Strengthen the bed-sleep association Sleep restriction • Reduce time in bed to actual sleep time • Improves sleep efficiency and strengthens bed-sleep association • Avoids disrupted and fragmented sleep
What can be done? Relaxation • Progressive muscle relaxation/yoga/Alexander technique • Breathing exercises • Mindfulness • Imagery Cognitive techniques • Thought blocking • Listing the positives • Turning the tables • Trying to stay awake • Alternative thinking techniques • Carefree attitude towards sleep • Test the hypothesis • Consider cognitive behavioural therapy and related techniques
What can be done? Relaxation • Progressive muscle relaxation/yoga/Alexander technique • Breathing exercises • Mindfulness • Imagery Cognitive techniques • Thought blocking • Listing the positives • Turning the tables • Trying to stay awake • Alternative thinking techniques • Carefree attitude towards sleep • Test the hypothesis • Consider cognitive behavioural therapy and related techniques
But what about medication? • Many on the market • Frequently employed • Intended as short term aid but often become long term crutch • Daytime side effects • Treating a symptom, not the cause • Perhaps more useful as an ad hoc adjunct, for acute problems
Conclusion • Insomnia is not a life sentence • Seeking help is the first step towards moving forward • The ability to succeed comes from within but gaining support will increase your chances of doing so • Positive thinking is key • Believe!
"If you think you'll lose, you're lost,For out in the world we findSuccess begins with a fellow's will;It's all in the state of mind.Life's battles don't always goTo the strongest or fastest man;But soon or late the man who winsIs the man who thinks he can."Walter D. Wintle
thegoodsleepprogramme take charge, move forward, live life